

Full Length Research Article
The effect of TGF-β1 gene expression on patients with rheumatoid arthritis
Inam Tahseen Alwan*
Adv. life sci., vol. 12, no. 3, pp. 483-489, August 2025
*- Corresponding Author: Inam Tahseen Alwan (Email: enamt81@gmail.com)
Authors' Affiliations
[Date Received: 14/12/2024; Date Revised: 16/01/2025; Available Online: 31/10/2025]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: A systemic autoimmune disease, rheumatoid arthritis (RA), affects a wide range of ages and populations worldwide. In chronic RA, lymphocytes, synovial cells, antigen-presenting cells, their cytokines, and most importantly, Transforming Growth Factor-β1 (TGF-β1) are the leading players. The most critical for angiogenesis, immunosuppression, fibrosis, and chronic inflammation is TGF-β1, a potent anti-inflammatory mediator in RA with high expression at the site of RA.
Methods: A total of 53 rheumatoid arthritis (RA) patients (anti-CCP and RF positive) and 18 age- and sex-matched healthy controls were recruited using purposive sampling. Patients were enrolled from Al Zahraa Hospital, Al Karama Teaching Hospital, and affiliated clinics in Wasit Province. Inclusion criteria comprised confirmed RA diagnosis according to ACR/EULAR 2010 criteria, while patients with other autoimmune, infectious, or chronic inflammatory diseases were excluded. Ethical approval was obtained from the institutional review board, and informed consent was secured from all participants. Blood samples were collected for TGF-β1 gene expression analysis using RT-qPCR. Erythrocyte sedimentation rate (ESR) was determined, and disease activity was classified using the DAS28 score.
Results: RA patients showed significantly higher TGF-β1 expression than controls (ΔΔCt = −0.9 ± 2; t(52) = −3.28, P = 0.0019), corresponding to a geometric mean fold change of 1.87 [95 % CI: 1.28 – 2.71]. The expression of TGF-β1 on leukocytes did not vary significantly between males and females. Furthermore, TGF-β1 gene expression did not change amongst patients with low, moderate, and high disease activity levels.
Conclusion: The elevated level of TGF-β1 in the contemporary study might be correlated with RA in Iraqi patients. This relationship seems independent of gender and disease activity status and highlights the importance of TGF-β1 in RA pathogenesis, indicating its possible contribution as a disease detection biomarker. The implications of these findings are significant for understanding the molecular mechanisms underlying RA and may influence future therapeutic strategies.
Keywords: Rheumatoid arthritis, TGF-β1, Expression, Cytokines, Autoimmune disease
Introduction![]()
Rheumatoid arthritis is an idiopathic autoimmune illness characterized by persistent arthritis, leading to bone and cartilage degradation [1]. It mostly affects the synovial joints’ fullness and is linked to socioeconomic burdens, unsatisfactory mortality, and progressive impairment [2].
Furthermore, rheumatoid arthritis patients had a life expectancy shortened by 5–10 years. TGF-β1 is known to decrease inflammatory responses in RA, and the transforming growth factor is a homodimer with bidirectional effects in immune responses, inflammation, repair, and embryonic development [3]. Several studies have shown that TGF-β1, the transforming growth factor that controls fibroblast activity, is contained in the synovial fluid and tissue of RA patients. This factor is considered important in the pathophysiology of RA [4]. A cytokine called transforming growth factor-β1 is crucial for both healthy joints and those afflicted by osteoarthritis, the most prevalent condition [5].
Women and the elderly are more commonly affected by the general inflammatory disease, Rheumatoid arthritis (RA), than men [2]. Sjögren’s syndrome and rheumatoid arthritis are believed to be preponderant in women since females are cyclical in their hormonal cycle. Rheumatoid arthritis involves the synovial membrane because it is located in the joints; therefore, it causes continuous inflammation in as many joints as possible. The synovium, a thin tissue that covers tendons and joints, is usually involved in weight bearing, flexibility, and movement. The pathological processes that take place in rheumatoid arthritis, compared to the normal processes of joint friction, are illustrated. Inflammation leads to changes in the synovial membrane in individuals affected with rheumatoid arthritis, which erodes the bone and cartilage in the damaged joint. Rheumatoid arthritis is said to affect women between the ages of 40 and 60 more than men because of hormonal changes that occur following menopause. Many older women consider estrogen and progesterone to be a defense mechanism for bones and joints, which play a role in this protection, but these two hormones are minimized during menopause. Higher quantities of estrogen might act as protective measures against RA and SS because they could reduce inflammation from upregulated regulatory cytokines, including IL-10 and TGF-β [6]. Males and females at birth have twenty-two sets of somatic chromosomes as well as one set of sex chromosomes—the sex determining factor [7]. Autoimmune diseases are those diseases that result from the immune system’s inability to distinguish between normal body tissues and pathogenic antigens. Concerning the issue, it is important to note that TGF-β1 is synthesized as a latency-associated peptide and needs to be activated to exert its biological activity [8,9].
Methods![]()
This research involves 53 patients who were both anti-CCP-positive and RF-positive, and 18 healthy controls, who will be taken as the normal control. Disease severity was assessed using the DAS28 score in patients aged twenty-two to ninety-three years. Also, the patient’s E.S.R. was determined in a laboratory for each patient using the Wintrobe gravitational method. Patient demographics: sex, the severity of the illness, the illness duration, the treatment line, and associated diseases were recorded. The healthy subjects also did not have any pathological disease or history of cancer, immunological disorders, or any systemic diseases at the time of the research. Two milliliters of blood were drawn from each rheumatoid factor-positive patient and control subject. Serum was then separated and transferred into gel tubes.
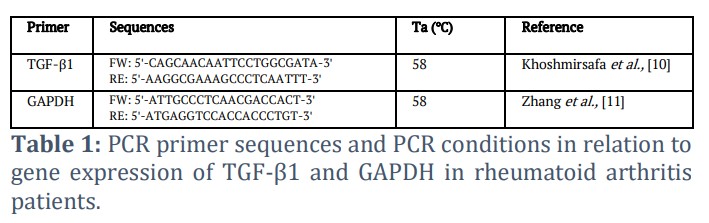
The table shows the FW and RE primer sequences for RT-qPCR of TGF-β1 and the reference gene, GAPDH. Listed primers were selected utilizing earlier tested and validated studies as references. The best annealing temperature (Ta) for both primer sets was determined to be 58 °C. GAPDH was used for the normalization of gene expression data. The sequences used in this study for TGF-β1 and GAPDH are shown in Table 1. The forward (FW) and reverse (RE) primer sequences are shown in this table, which are used for RT-qPCR analysis of the housekeeping gene GAPDH and TGF-β1. Primers were selected from previously validated studies as referenced. The annealing temperature (Ta) for both primer sets was optimized at 58 °C. GAPDH served as an internal control for the normalization of gene expression data.
TGF-β1 analysis
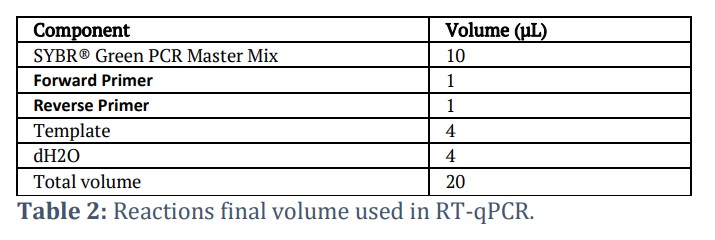
Peripheral blood samples were collected from patients diagnosed with RA and control individuals. Total blood RNA was extracted from patients and control individuals using the AccuZol reagent. The complementary DNA (cDNA) was reverse transcribed from RNA using an RT FDmix (Hexamer) kit, and the procedure was done in a reaction volume of 25 μL as per the manufacturer's instructions. cDNA was run in Real Time PCR for many cycles. The data were normalized to a housekeeping gene (internal control group), GAPDH. TGF-β1 expression gene was measured to detect the quantity of the above gene in patients and compared with healthy individuals as a control group using qPCR. The final volume used in RT-qPCR is shown in Table 2.
These components were the full reaction mixture composition used for quantitative real-time PCR analysis. To maximize the reaction, all reagents are used at their relative concentrations based on the final volume of the reaction: 20 μL per sample. A fluorescent detection system (SYBR Green PCR Master Mix, Applied Biosystems, USA) was used for amplification monitoring. The template is cDNA, which was made from the patient and control RNA samples.
Statistical analysis
Quantitative expression levels were calculated from ΔCt values and analyzed using the 2⁻ΔΔCt method. Because raw replicate Ct data for GAPDH were unavailable, its variability could not be determined. GAPDH values are therefore reported descriptively as the internal reference, and no statistical testing was applied to its Ct values.
Results![]()
Study of cytokines TGF-β1 gene expression in RA patients
This research used Real-Time PCR with SYBR GREEN. All double-stranded DNA, including cDNA, was identified by the luminous dye, and the amplification was documented as a cycle threshold (Ct) value. A lower Ct number signifies a greater quantity of the target, and conversely, a higher Ct value suggests fewer copies. High Ct values signify decreased gene expression, while low Ct values imply elevated gene expression [11-13]. The gene expression of TGF-β1 was studied by QPCR in this study, using the method (Livak & Schmittgen, 2001). The fold variations were calculated, and real-time PCR outcomes were converted to mRNA.
Assessment of mRNA expression of TGF-β1 in RA patients and the control group
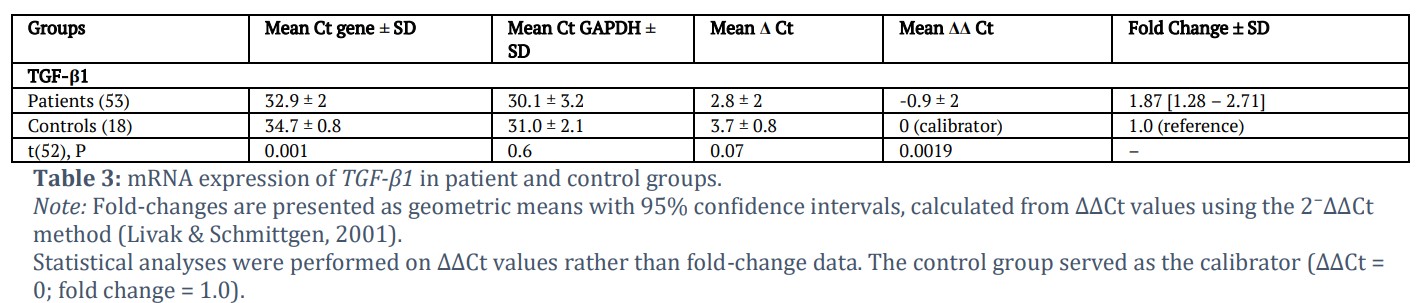
Table 3 showed a significant difference in TGF-β1 mRNA expression levels between the patient group and the controls. The exact enhancements of gene expression rates were determined by PCR analysis. As per the present research work, TGF-β1 expression was approximately 1.9-fold higher in RA patients than in controls (P = 0.0019). The results revealed that levels of Cytokines and other inflammatory mediators are highly significant in chronic inflammation and rheumatoid arthritis. [14].
Thus, these observations corroborate other published work by Khoshmirsafa et al., [10], which indicated an increase in TGF-β1 content in blood and synovial tissue in RA patients. The implication of TGF-β1 in the pathogenesis of rheumatoid arthritis is clearly manifested in many articles comparing the concentration of TGF-β1 in synovial fluids of RA patients and those of normal individuals; the concentration being higher in the former [15]. Another study showed that there were increased levels of active TGF-β1 in rheumatoid arthritis patients’ synovial fluid [5]. However, RA patients, whether at the time of diagnosis or those who have been treated with DMARDs, also had higher plasma concentrations of TGF-β1 than the normal control group [1].
In Table 3, a comparison of TGF-β1 mRNA levels of RA patients (n = 53) and healthy persons (n = 18) by real time RT PCR is shown. Quantitative PCR data are represented by mean Ct values of TGF-β1 and GAP reference gene, and normalized expression values as ΔCt, ΔΔCt, and fold changes. Differences between the patient and control groups were compared, and the p-values associated with each parameter were presented. All results are shown as mean ± SD in order to compare the level of TGF-β1 expression between all groups.
Assessment of mRNA expression of TGF-β1 in RA patients based on their gender
The comparison data of male and female RA patients for the mRNA expression of TGF-β1 is summarized in Table 4. The present work’s data showed that TGF-β1 expression in males was 5.5 ± 8.6 and in females was 4.9 ± 7.4. Gene expression of TGF-β1 was non-significantly different between the male and female RA patients. Pandya et al., [16] exhibited no significant disparity in chemokine levels between female and male patients. Furthermore, Panoulas et al., [17] indicated that no significant differences were detected between the control group and patient group. These two groups, before and after adjustments for age and sex, regarding the IL6 or TGF-β1 genotypes and alleles, were examined. The dual function of TGF-β1 has been extensively investigated in relation to malignancies and autoimmune diseases. The inclusion of the TGF-β1-509 T allele in the genotype (CT + TT) may constitute a risk factor for young-onset rheumatoid arthritis in female individuals. Certain investigations demonstrated markedly elevated IL-10 and reduced TGF-β1 blood levels in women with rheumatoid arthritis compared to the control group [18].
Assessment of mRNA expression of TGF-β1 in patients with RA based on disease activity
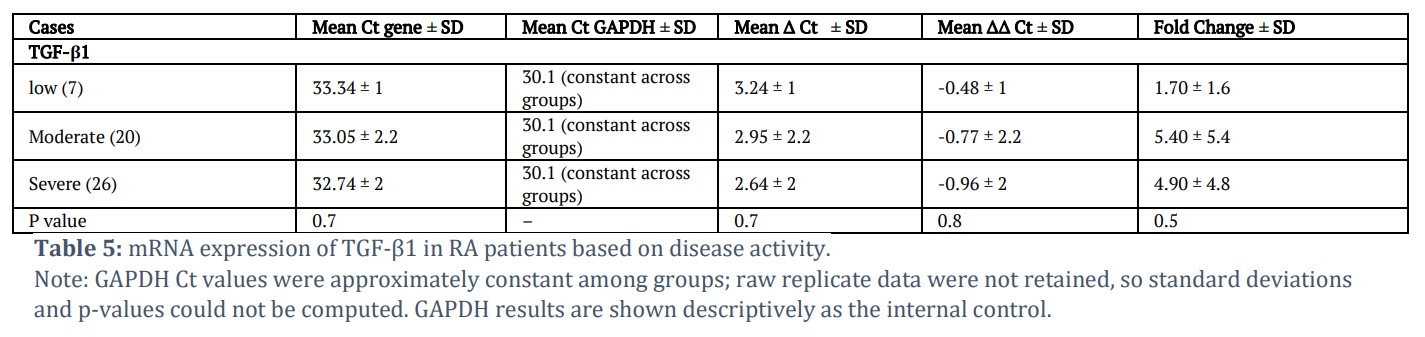
The differences in TGF-β1 mRNA expression across RA patients are tabulated in Table 5 according to the activity of the disease. The findings showed the distribution of TGF-β1 expression in three disease activity categories: low activity (1.70 ± 1.6), moderate activity (5.40 ± 5.4), and severe activity (4.90 ± 4.8), with no discernible variations between the three groups. The work of Janssens et al., [19] reported that TGF-β1 is highly expressed during fracture healing. In an article by Cho et al., [20], however, the authors argued that the role of TGF-β1 is not limited to the development and turnover of bone but extends up to the process of bone repair. Therefore, TGF-β1 is one of the growth factors that are considered for use as a bone-forming agent in the promotion of fracture healing or the prevention of excessive bone resorption in osteoporosis. On the other hand, Kooloos et al., [21] stated that TGF-β1 is believed to suppress the inflammatory response in the blood of RA patients. Contradictory results have been stated regarding the functionality of the SNP TGF-β1 869T > C in reducing or increasing the production of the enzyme [22,23].
In a different study, T in the T869C polymorphism may mean relatively low TGF-β1 production and is associated with the rate of the disease. Due to having less of this anti-inflammatory cytokine, RA patients may experience more inflammation [24]. In another study, TGF-β1 was detected together with upregulated TC / PC of TGF-β1 discharging THBS1 and improved TGFBR1 in RA synovial fibroblasts (SFBs). This implies prospects of TGF-β1-induced effects, including MMP-mediated matrix degradation/remodeling, have (autocrine) pathogenic relevance in RA patients [25]. T/C869 and G/A800 genotypes of the TGF-β1 gene have also been demonstrated to affect the severity of RA and increase Osteoporosis risk in T and A allele carriers with T/C869 and G/A800 gene polymorphisms, respectively [26]. RSF are known to produce higher levels of TGF-β1 and its receptor TGF-βRI, and the correlation observed between disease activity indices of inflammation supports the role of TGF-β1 in inflammation [3]. Zhou et al., [27] found that TGF-β1 level in the blood was reduced; however, there was no statistical relation between the -509 C/T polymorphism of TGF-β1 and the risk and severity of RA.
Such a cytokine is TGF-β1, which has been described both as supporting inflammation and as anti-inflammatory. TGF-β1 takes part in many biological functions, mainly in growth and development, inflammation, host defense, and tissue repair. TGF-β1 is secreted by the inflammatory cells as a member of the cytokine family. As a protective factor, TGF-β1 helps in the repair of tissues and the clearance of inflammatory reactions. However, in the cytokine network growth factor, as we have seen, this must be in an optimal amount for those defensive actions to happen in an orderly manner [28].
Table 5 shows the proportion of comparative measurements of TGF-β1 mRNA in rheumatoid arthritis patients depending on disease activity frequency. The study population was categorized into three groups: they are; low disease activity, moderate disease activity, and high disease activity. This was followed by quantification of the relative expression levels by real-time PCR, while the internal control housekeeping gene used was GAPDH. Data are shown as mean Ct values and corresponding ΔCt/ΔΔCt and fold change between activity groups. The GAPDH Ct values reported in Tables 4 and 5 appear inconsistent (identical means with SD = 0 and p < 0.001). The underlying data should be re-examined and the statistical analysis recalculated to ensure accurate representation of reference gene variability.
Figures & Tables

As expected, higher levels of TGF-β1 are established in RA patients in the present study in comparison with previous studies. Numerous investigations have shown that there is an elevated level of TGF-β1, both in serum and synovial tissue, in RA patients [10]. A contribution of TGF-β1 to RA has been evidenced by studies that revealed higher levels of TGF-β1 in the synovial fluids of RA patients [15].
Thus, the absence of an observed male-female difference in TGF-β1 expression supports similar findings documented earlier. The same study design was used to investigate the levels of chemokines [16], and no significance was noted for TGF-β1 genetic constitution and alleles comparing patients and controls after matching with age and sex [17].
As for constructive components of the genotype, our data did not reveal convincing links between TGF-β1 expression and disease activity. This discovery has added a layer to the already extensive understanding of the role that this protein, TGF-β1, plays in RA. Studies carried out in the past reveal that TGF-β1 is synthesized during the healing of fractures [19] and is critical in the growth and remodeling of bones [20]. It has been mentioned that cytokines can have antagonist roles, which concern the inactivation of inflammation [21] and in other ways [25].
There is evidence of a multifaceted part TGF-β1 plays in human RA since it is involved in both anti-inflammatory and pro-inflammatory behaviors. It promotes resolution of inflammation and tissue healing whilst used in correct proportions and optimizes defensive mechanisms [28]. It is suspected that this accounts for the ability to detect raised TGF-β1 concentrations at both stages of the disease activity.
The present work is useful for understanding the effects of TGF-β1 in rheumatoid arthritis of Iraqi patients. In the context of the present investigation, it was confirmed that TGF-β1 gene expression was higher in RA patients than in healthy controls (ΔΔCt = −0.9 ± 2; t(52) = −3.28, P = 0.0019), corresponding to a geometric mean fold change of 1.87 [95 % CI: 1.28 – 2.71]. This finding corresponds to data from the literature indicating that TGF-β1 concentrations are elevated in serum and synovial lining membrane of RA patients, supporting the hypothesis that it can take part in the pathogenesis of the disease.
Interestingly, in the present study, it was found that expression of TGF-β1 was not related to either sex or the disease activity of the RA patients. There were no substantial variations in male and female patients’ TGF-β1 expression, which hints that the cytokine may play a gender-independent role in RA. In the same manner, when the patients were divided based on the disease activity, no difference was found in TGF-β1 levels, suggesting that this cytokine is elevated irrespective of the severity of the disease.
These data help to advance knowledge of molecular-level changes in RA and indicate TGF-β1 as a potential RA diagnostic marker that is operative irrespective of the patient’s gender and inflammation. These considerations, as well as the observed increase in the level of TGF-β1 in most subgroups of patients, allow us to conclude that this cytokine is more likely to be involved in the disease process than as a marker of disease progression. Further investigations should be directed at determining the role of TGF-β1 in the pathogenesis of RA and whether it is a novel target for treatment.
The importance of the clinical relevance of this discovery becomes obvious when giving attention to the fact that the level of TGF-β1 could be useful in the diagnosis of RA and may perhaps be useful in assessing the response of patients to treatment, yet it may not be particularly useful in determining the severity of the disease. More investigations, including the control of a higher number of patients and longitudinal research approaches, should be conducted to confirm these observations and to determine their treatment-related consequences. The absence of replicate variability data for GAPDH limits assessment of reference-gene stability; however, this does not affect ΔCt-based relative quantification of TGF-β1 expression.
Acknowledgement
Special thanks to Dr. Kareem Hamed Ghali, Dr. Kahtan Adnan Hafedh, D.R.M.R. Specialist of Rheumatology & Medical Rehabilitation in Al-Karama Teaching Hospital, Dr. Jalal Tuffah, Aqeel Naji, and Ali Abd Al-Kadhum of Al Kut Teaching Hospital, and Inass Tahseen of Wasit Health Department for their infinite assistance. We are thankful to Dr Safaa Abdullah of College of Medicine, Wasit University, for assisting us in the result analysis.
Author Contributions
Inam Tahseen Alwan theorized, supervised, reviewed the article, executed the literature search, and provided important input during the preparation of the manuscript.
The author(s) declare that there is no conflict of interest.![]()
References
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0

