

Review Article
Non-Surgical Treatment Methodologies and Prevention for Malignant Melanoma
Honggang Yu1, Rizwan Ali2*, Rui Lei2, Jinghong Xu2
Adv. life sci., vol. 11, no. 1, pp. 07-17, February 2024
*– Corresponding Author: Rizwan Ali (12018636@zju.edu.cn )
Authors' Affiliations
2. Department of Plastic Surgery, The First Affiliated Hospital, School of Medicine, Zhejiang University, No. 79 Qingchun Road, Hangzhou 310003 – China
[Date Received: 10/04/2023; Date Revised: 03/10/2023; Date Published: 25/02/2024]
Abstract![]()
Introduction
Methods
Discussion
Conclusion
References
Abstract
Melanocytes in the skin and other organs generate the tumor known as malignant melanoma (MM). It has a high degree of malignancy, a deprived prognosis, and a propensity for local recurrence and distant metastasis. Although there have been tremendous advancements in MM management choices over the past ten years, there are still a dearth of clinically viable therapy alternatives and no internationally accepted treatment standard. The prognosis of MM patients has recently improved thanks to the development of immunotherapy and targeted therapy. As a result, this article examines the most recent findings from studies on the non-surgical treatment methodologies for MM and its preventive measures.
Keywords: Malignant melanoma; Treatment therapies; Combined therapies; Prevention
Introduction![]()
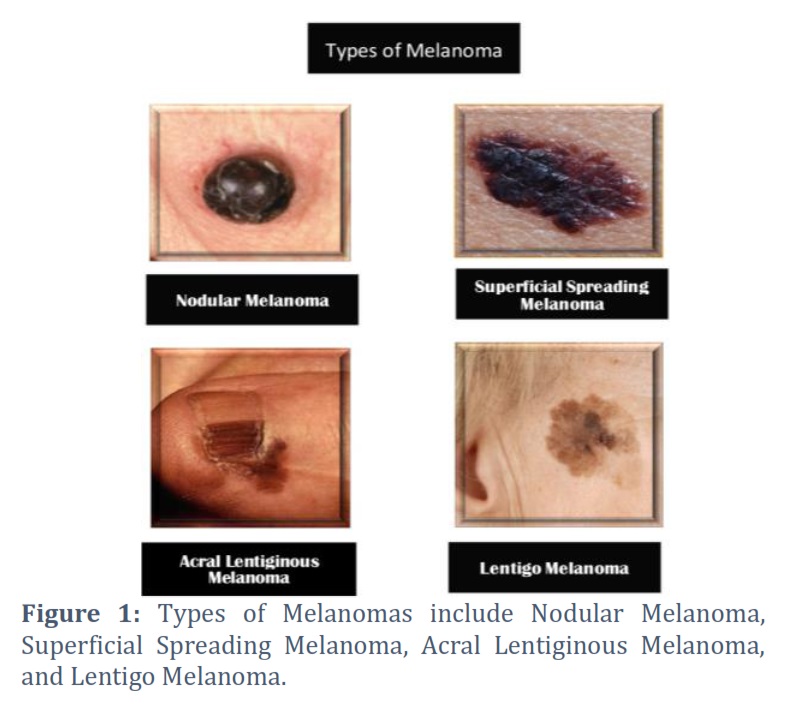
Malignant melanoma (MM) is a tumor produced by melanocytes of skin and other organs. It is one of the most severe types of skin cancer, ranked fifth among men and sixth among women in the United States for the frequency of cancer diagnoses [1,2], while there are about 20000 new cases in China every year [3]. Malignant melanoma represents merely 1% of all skin cancers [4]. In 2020, over 300,000 individuals received melanoma diagnoses worldwide, with over 50,000 patients succumbing to MM globally [5]. Conventional melanomas encompass four distinct types, namely nodular, superficial spreading, acral lentiginous, and lentigo melanoma (Fig. 1). A tiny biopsy specimen makes this categorization difficult. According to research, the prognosis of various melanoma types varies; however, multi-variation analysis has less impact on the histological types of melanomas [6-8]. Pathological reports provide the basis for this categorization [9]. Except for lung cancer, melanoma incidence is rising more quickly in women than in other neoplasms [10]. Also increasing every day is the death rate. Nowadays, metastatic melanoma claims one life every four hours. Compared to other cancers, which often affect older individuals more than younger ones, melanoma negatively affects more people in their 20s and 30s. Melanoma is often diagnosed at a median age of 57, and the average age at death is 67. According to skin biopsies, melanoma in youngsters is becoming more common. Men are more prone than females to acquire melanoma. Males often get melanoma on their backs, whereas females typically develop it on their arms and legs [11]. While the five-year relative survival rate for all MM stands at 92%, it drops significantly for localized lesions and distant metastases, with rates of only 65% and 25%, respectively. Approximately 4.3% of melanoma patients develop metastasis [12]. Melanoma incidence is quickly rising globally, becoming a serious public health issue [9]. Surgery is the first choice for the treatment of non-metastatic MM. However, considering the anatomical location, the number of lesions and the rate of recurrence after surgery, surgery is not suitable for all patients with MM. For the above situation, the development of new drugs for selective targeting and immunotherapy has improved the response rate, and immunization and targeted therapy are effective strategies for treating MM. The hazard of melanoma to the general public's health is reduced by taking the proper preventative measures. The objective of this article is to go over the non-surgical treatment methodologies for malignant Melanoma and its preventive measures.
Methods![]()
Literature Search and Selection Criteria
In order to gather relevant information, a comprehensive literature search was conducted using PubMed and Google Web Browser. Key terms such as “types of melanomas,” “treatment therapy of skin cancer or melanoma,” “non-surgical treatment of malignant melanoma,” “prevention of skin malignant melanoma” and “latest treatment therapy of skin malignant melanoma” were utilized. The search results were carefully evaluated to ensure their relevance to the topic at hand. From the initial pool of literature, a total of 61 peer-reviewed research articles were selected for inclusion in this study.
Discussion![]()
Treatment therapies
Immunotherapy
Malignant melanoma poses a formidable challenge in oncology, characterized by rapid dissemination and early metastasis formation. Despite extensive efforts in recent decades, conventional therapeutic approaches such as chemotherapy and radiotherapy have yielded limited success due to melanomas' inherent resistance. Consequently, there is a growing emphasis on exploring novel immunotherapeutic agents to enhance clinical responses in melanoma patients [13]. Systemic drug therapies, notably immune checkpoint inhibitors, have significantly improved melanoma survival rates since a series of pivotal approvals starting in 2011 [14]. Immunotherapy is a term used to describe a type of treatment whereby the body's immune system is intentionally stimulated or suppressed to treat illnesses that arise from either a high or low immunological status. A high occurrence rate in individuals with compromised immune systems, active lymphocyte infiltration in both primary and metastatic malignancies, and melanoma antigen recognition by infiltrating T lymphocytes are the hallmarks of MM. Immunotherapy spans four key categories. The first classification involves biological immunotherapy, incorporating agents like cytokines, interferon, and granulocyte-monocyte colony-stimulating factor. The second category centers on vaccination, utilizing peptides, whole proteins, viruses, DNA, or dendritic cells (DC). The third category encompasses adaptive cell therapy (ACT), employing lymphocyte activated killer cells (LAK), tumor-infiltrating lymphocytes (TIL), and other specific lymphocytic cells. The fourth category revolves around immune checkpoint blockade.
In recent years, the immunological basis of malignant tumors has prompted the identification of antibodies directed at specific targets. The focus of this immunotherapy primarily lies in the targeted disruption of the anti-regulatory mechanisms within the immune response. Noteworthy examples include anti-programmed cell death 1 (PD-1) and anti-cytotoxic T lymphocyte-associated antigen-4 (CTLA-4). These inhibitors significantly enhance and prolong the overall survival rates of patients with metastatic melanoma (MM) [15].
Bio-immunotherapy
The most common drugs in biological immunotherapy are high-dose interleukin-2 (IL-2) and interferon. IL-2 demonstrates the capacity to stimulate various lymphocyte subsets, including natural killer cell (NK) cells, effector CD4+T and CD8+T cells, and regulatory T cells, playing a crucial role in immune homeostasis. Bio-immunotherapy is commonly employed in conjunction with targeted radiotherapy, vaccines, or anti-CTLA-4 antibodies. However, this combined approach lacks comprehensive verification, and as of 2011, only a singular preparation had received approval beyond clinical trials [16]. The therapeutic application of IL-2 is constrained by adverse events, such as capillary leakage syndrome, mediated by the high-affinity interaction of IL-2 receptors. IL-2 treatment exhibits a low response rate (<10%), severe multiple organ toxicity, and only a minority of patients achieve long-term disease-free responses [17]. Apart from enhancing immune responses and effector cell functions, the GITR pathway is considered a promising immunotherapy target due to its potential to alleviate regulatory T-cell suppression [18]. Nonetheless, substantial clinical improvement has not been observed. An ongoing phase I study is exploring the effects of the GITR pathway stimulator TRX518M, either alone or in combination with gemcitabine, pembrolizumab, or nivolumab [18]. The costimulatory receptor 4-IBB on immune cells supports the development of effector T cells and the discharge of cytokines. Phase I research has reported the tolerability of two 4-IBB agonists, urelumab, and utomilumab [18]. CD27, also known as TNFRSF7, significantly aids T-cell activation, promoting T-cell proliferation and differentiation. An antibody that is a CD27 agonist, varlilumab, has promising activity in several malignancies. The combination of varlilumab + nivolumab or atezolizumab is currently being studied [18]. Therefore, biological immunotherapy needs further research.
Vaccination
The vaccine against MM cells is an active and specific immunotherapy using melanoma cells removed by patients themselves. DC is an antigen-presenting cell that can improve the ability to induce T cell immunity by activating cytotoxic T cells and pro-inflammatory cytokine responses. Therefore, DC can be used as a vaccine, but the efficacy of DC-based vaccines is limited. Certain research has indicated that viruses possess the capability to infect cells, triggering an immune response, and can be harnessed for oncolytic purposes. This method activates the immune system against tumors by releasing cytokines and other regulatory molecules. Examples include adenovirus, herpes simplex virus, retrovirus, and measles virus [19]. Studies have shown that modifying the neurotoxicity of herpes simplex virus leads to the death of human MM cells and targeted replication in MM tissues of nude mice. Safety was confirmed in a phase I clinical trial involving intradermal injection for MM patients [20] .
Herpes simplex virus type 1 serves as the basis for the oncolytic immunotherapy talimogene laherparepvec (T-VEC). T-VEC selectively replicates in tumors, prompting the production of granulocyte-macrophage colony-stimulating factor (GM-CSF), activating the immune system to combat the tumor. T-VEC is the sole oncolytic viral treatment explored in randomized clinical studies [21].
T-VEC's effectiveness was first demonstrated in a phase II study with 50 patients. They received T-VEC every three weeks for different metastatic conditions, including visceral metastases (n = 24), skin- or lymph node-only metastases (n = 16), and unresectable regional disease (n = 10). The study recorded a 26% overall response rate (ORR). Additionally, both treated and untreated lesions showed therapeutic effects, and instances of disease progression before the response, termed "pseudo-progression," were observed [22]. In phase III clinical trials for melanoma therapy, T-VEC demonstrated success. The study involved 436 patients with unresectable injectable melanoma who were randomly assigned to receive either intralesional T-VEC (n = 295) or subcutaneous GM-CSF (n = 141). The T-VEC group exhibited a statistically significant improvement in the illness compared to the GM-CSF group, with an overall response rate (ORR) of 26.4% (p 0.001). Commonly reported adverse events included pyrexia, chills, and fatigue [21]. In the OPTiM phase III randomized study with a 2:1 ratio, patients receiving T-VEC demonstrated a higher overall response rate (ORR) compared to those receiving GM-CSF (26.4 vs. 5.7%, p < 0.0001). Cellulitis was reported as the sole adverse event in just over two patients [23].
The primary advantage of oncolytic viruses lies in their ability to directly target tumor cells and propagate. Current research focuses on enhancing the virus's selective replication for tumors and improving its immune stimulation capabilities, thereby offering a multimodal approach to treat tumors. While DNA vaccines have demonstrated safety and immunogenicity in clinical trials, their efficacy has not yet met satisfactory results [24]. The exploration of effective vaccine treatment for MM is still in progress.
Adaptive cell therapy (ACT)
Adoptive cell therapy (ACT) involves gathering lymphocytes from either the patient's blood or tumor, followed by in vitro selection, expansion, and activation of these cells. Subsequently, modified lymphocytes are reintroduced into the patient to stimulate an immune response against cancer. The primary cell types utilized in ACT include peripheral blood lymphocytes, tumor-infiltrating lymphocytes (TIL), and lymphokine-activated killer cells (LAK). The use of ACT has achieved good results, but it is still at the experimental level. Before it is considered as a safe and effective strategy, it still needs to be further improved step [25]. A new method of ACT is to infuse isolated and expanded autologous CD4+T cells, which activate MM associated antigen. This treatment needs to develop a specific treatment plan of “customized medicine” for each patient; furthermore, extensive cell culture periods, the expertise of trained personnel, and meticulous patient preparation are essential requirements [26]. Certain research indicates that chemotherapy-induced reactive myelogenesis, resulting from lymphatic depletion, constrains the effectiveness of ACT. Lymphatic depletion triggers the mobilization of hematopoietic progenitor cells, leading to their differentiation into immunosuppressive myeloid cells, causing a notable surge in peripheral myeloid cells. Notably, interleukin-6 (IL-6) has been identified as a factor promoting the differentiation of hematopoietic progenitor cells into peripheral myeloid suppressor cells following lymph depletion. This process reduces the survival and immunosuppressive capabilities of tumor-infiltrating lymphocytes (TIL). In the mouse model receiving ACT, IL-6 reduced the growth of tumor, but the inhibitory cells from peripheral myeloid system may lead to the failure of ACT [27]. However, a significant limitation of this strategy is the cost, time, and technologies necessary. There are currently clinical trials testing checkpoint inhibitors and ACT [28].
Blocking of immune inspection station
The development of correct immune response is based on some immune checkpoints, which can prevent some self-directed activities of autoimmunity. In MM, immune checkpoint blockade therapy is targeted at molecules over-expressed in MM, such as PD-1 or CTLA-4.
PD-1, a cell surface molecule known for its inhibitory properties, is expressed by activated T, B, and NK cells, dampening effector functions. Studies demonstrate that PD-1/PD-L1 inhibitors in multiple myeloma (MM) can selectively bind to PD-L1 on tumor cells, inhibiting its expression. This process facilitates the restoration of suppressed T-cell functions, allowing them to regain their ability to recognize tumor cells. Consequently, this autoimmune response contributes to the anticancer effects. Notably, in 2014, the US Food and Drug Administration approved PD-1 inhibitors such as nivolumab and pembrolizumab for treating advanced unresectable or metastatic MM. Over the span of a few years, the FDA greenlit six PD-1/PD-L1 inhibitors for commercial distribution and their application in treating and researching MM [29]. Navuzumab’s interaction with MM’s PD1 and its ligands PDL-1 and PDL-2 has demonstrated noteworthy clinical efficacy, particularly in melanoma. The initial evaluation of Navuzumab took place in the CheckMate-238 clinical trial in March 2015. This trial, a randomized, controlled, double-blind phase III study [30], aimed to compare the efficacy of Navuzumab (administered at 3 mg/kg every two weeks) with Epizumab (administered at 10 mg/kg every three weeks for four cycles) as adjuvant therapy for resectable stage III B/C or IV MM. The study encompassed 906 patients, meticulously matched in a 1:1 ratio. Findings revealed that the 12-month relapse-free survival rate (RFS) for the Navuzumab group reached 70.5%, surpassing the 60.8% rate observed in the Epizumab group. Notably, the incidence of grade 3 to 4 adverse reactions was markedly lower in the Navuzumab group (14.4%) compared to the Epizumab group (45.9%). Additionally, the Navuzumab group experienced a lower rate of treatment interruption due to adverse events, standing at 9.7%, in stark contrast to the 42.6% recorded in the Epizumab group. There were 2 cases of death due to adverse drug reactions in the epizumab group.
In a phase I study, Bevacizumab and imatinib demonstrated safety in individuals with metastatic melanoma [31]. A multicenter phase II study explored the effectiveness and safety of carboplatin-paclitaxel with bevacizumab as the initial treatment for patients with unresectable metastatic melanoma, involving a total of 50 participants. Common adverse events (AEs) included peripheral neuropathy, fatigue, hair loss, and gastrointestinal issues, with an observed overall response rate (ORR) of 34% [32]. Concluding the trials, the AVAST-M phase III randomized trial, investigating bevacizumab’s adjuvant treatment efficacy in melanoma patients, is currently underway at multiple centers [33]. WEBER et al. [34] also focused on the importance of Navuzumab and Pamuzumab in the treatment of MM. Their study revealed a rapid decrease in PD-1 and regulatory T cells post-treatment initiation, leading to a reduced risk of disease progression and metastatic spread [34]. Another down-regulated signal emerges through the interaction between CTLA-4 and activated T cells, hindering the transcription of IL-2 and impeding the cell cycle's progression. Epizumab, a recombinant human monoclonal antibody, effectively enhances T lymphocyte proliferation and activation by blocking the interaction between CTLA-4 and its ligand, the B7 molecule.
In 2011, the U.S. Food and Drug Administration sanctioned the use of Pizumab for metastatic or non-resectable multiple myeloma (MM) patients. In a phase III clinical trial involving 197 MM patients who had previously experienced treatment failure, epizumab, gp100 peptide vaccine, and a combination of both were administered. The outcomes indicated clinical benefit rates of 5.7%, 1.5%, and 0.9%, respectively, with corresponding median survival times of 10 months, 6.4 months, and 0.1 months [35].
Serine-threonine protein kinase/mitogen activation (BRAF/MEK) inhibitor
Approximately 50% of MM patients carry mutations in the BRAF gene. Rajkumar et al. proposed that individuals with BRAF non-p. V600 mutant melanomas might derive advantages from the existing FDA-approved BRAF/MEK inhibitor combination therapy, typically designated for patients with BRAF p.V600 mutations [36]. In 90% of instances, this mutation results in the substitution of valine with glutamic acid (V600E mutation) at the 600th amino acid position of BRAF, while the remaining cases primarily involve an alternative substitution (V600K) at the same position [37]. Mitogen-activated protein kinases (MAPK) constitute a set of BRAFs responsive to various extracellular stimuli, including cytokines, neurotransmitters, hormones, cell stress, and cell adhesion. The presence of mutated BRAF induces the structural activation of the MAPK pathway, promoting heightened cell proliferation and contributing to carcinogenic processes.
Sorafenib, a tyrosine kinase inhibitor, inhibits BRAF and tyrosine kinase related with vascular endothelial growth factor (VEGF) and platelet-derived growth factor (PDGF). However, it is ineffective against BRAF with the V600E mutation, resulting in intolerable non-targeted effects during treatment. Furthermore, the combination of sorafenib with chemotherapy demonstrated no discernible benefits in two randomized phase III trials [38]. Hence, irrespective of the BRAF mutation status, sorafenib is not advised as a standalone treatment or in conjunction with chemotherapy for MM patients. Vemurafenib specifically targets the mutated BRAF kinase domain (V600E), with minimal impact on wild-type BRAF. Phase I and II trials demonstrated the significant efficacy of vemurafenib in individuals with advanced MM harboring the V600E BRAF mutation [39]. These findings were validated in the third phase of a randomized controlled trial, where 675 patients with untreated metastatic melanoma (MM) (95%) or stage IIIC MM (5%) were treated with vemurafenib or dacarbazine. The outcomes indicated a notably higher survival rate among MM patients treated with vemurafenib compared to those treated with dacarbazine [40]. In August 2011, the Food and Drug Administration granted approval for vemurafenib as both the first- and second-line treatment for tumor patients carrying the V600E mutation in BRAF [41]. Dabrafenib, functioning as a selective BRAF inhibitor, has demonstrated substantial effectiveness in phase I/II studies involving patients with metastatic melanoma [42]. Vemurafenib and dabrafenib underwent testing on melanoma (MM) patients with brain metastasis who had not received prior treatment. This marks the first clinically beneficial approach for individuals with brain metastasis. Notably, both vemurafenib and dabrafenib exhibit efficacy in patients carrying the V600K mutation; There is another non-V6 00E mutation in about 10% of BRAF patients, and the most common non-V6 00E mutation is V6 00K. At present, the efficacy of dabrafenib in patients with non-V600E mutations is being further studied [43]. The Ras/Raf/MEK/ERK signaling pathway, categorized as a MAPK pathway, has broad activation potential. This pathway facilitates the transmission of extracellular signals to the nucleus, instigating alterations in the expression profile of specific intracellular proteins, ultimately influencing cellular destiny. Compared with drugs that inhibit MEK and BRAF V600E/K mutations, MEK inhibitors can significantly improve the survival rate of patients. Recently, a phase III trial was published to compare trametinib, a selective allosteric MEK1/2 inhibitor, with dabrafenib, which was used to treat BRAF V600E/K target mutations. The findings indicated a substantial extension in the endpoint of the first remission for patients undergoing trametinib treatment [44]. Despite its efficacy against mutated BRAF in melanoma, trametinib exhibits a low response rate when used as a standalone medication, potentially restricting its future application in isolation [45].
IFN
IFN is a kind of cytokine with many biological activities. Type I IFN, especially IFN- α, it has the functions of immune regulation, anti-angiogenesis, anti-proliferation and pro-apoptosis, and is widely accepted and used for the treatment of stage IIB to III melanoma after surgery. However, there are still many problems to be considered about IFN treatment.
Primarily, there lacks a standardized criterion for the ideal dosage and treatment duration. At present, the standard drug administration scheme commonly used in treatment is composed of two stages, first of which is the high-dose IFN started within 4 weeks after operation- α Intravenous administration stage: 20 million U · (m2 · d) – 1, 5 days per week, for 4 weeks; The second is the subcutaneous administration stage of maintenance dose: 10 million U · (m2· d) – 1, 3 days a week, lasting for 48 weeks. However, commonly used regimens are not necessarily optimal. IFN- α decrease the relapse and improving OS is worth affirming, however, this effect was not significantly different with different dosing and courses of administration [46].
Secondly, the persistent challenge for physicians lies in managing the toxic effects of IFN. Despite attempts by researchers to modify the administration schedule to minimize adverse events (AEs) or enhance patients' eminence of life, the anticipated outcomes have not been realized. In contrast to the observation group, the 4-week HDI intravenous administration scheme exhibited comparable 5-year relapse-free survival and overall survival rates, albeit with a notable decline in the quality of life [47]. This shows that the effect of IFN has a great correlation with the length of treatment. Intermittent high-dose intravenous IFN- α 2b treatment basically retained the efficacy of HDI treatment scheme, and also significantly reduced the rate of AEs, but the recurrence-free survival (RFS) was notably inferior compared to the standard HDI treatment group [48]. It shows that intermittent administration cannot effectively inhibit the recurrence of tumor, so this scheme is difficult to promote.
Polyethylene glycol (PEG) IFN- α 2b is an IFN with a long half-life, which can improve the RFS of patients with stage III melanoma, but the effect on DMFS and OS is not supported by evidence. Its therapeutic effect and toxicity characteristics are generally similar to those of HDI. Although compared with IFN, a higher percentage of patients receiving PEG-IFN treatment stopped treatment due to toxicity, its advantages are also very obvious: longer half-life makes administration more convenient [49].
Combined therapy
BRAF inhibitor combined with MEK inhibitor
While BRAF inhibitor and MEK inhibitor combinations substantially enhance response rates and survival duration in advanced MM patients, approximately 50% of individuals exhibit drug resistance within approximately six months of receiving either BRAF or MEK inhibitor monotherapy [50]. There may be many mechanisms for this drug resistance. For example, the MAPK pathway can be reactivated after single treatment of BRAF inhibitors, resulting in NRAS, CRAF and MEK1/2 mutations and/or overexpression in patients; However, MAPK pathway reactivation is rare after MEK inhibitor monotherapy [51]. Therefore, the combined treatment of BRAF and MEK inhibitors may inhibit the activation of MAPK pathway more widely and persistently, avoid early drug resistance, and produce more significant and lasting anti-tumor effect. In 2014, the FDA granted approval for the combined use of trimetinib and daprofenib in treating non-resectable or metastatic advanced MM associated with BRAFV600E and V600K mutations. In a recent phase II clinical trial, patients with BRAF V600 mutant MM receiving the combined therapy of trimetinib and daprofenib exhibited a median overall survival time (mOS) surpassing two years. Additionally, the three-year progression-free survival rate and three-year overall survival rate were reported as 21% and 38%, correspondingly [52]. During the phase III clinical trial, a notable contrast in effectiveness emerged between the combined treatment group and the daprofenib-only group. Individuals in the combined treatment cohort exhibited a progression-free survival duration of 11.4 months, whereas the daprofenib-only group showed a comparatively shorter period of 7.3 months. However, there was no significant contrast in the occurrence of severe adverse events or the frequency of drug discontinuation between the two groups [53] . In addition, in 2015, the FDA also approved the combined treatment of corbitinib and vermorafenib. In conclusion, the concurrent administration of BRAF and MEK inhibitors not only enhances response rates and extends survival effectively but also maintains manageable overall toxicity without a significant rise compared to single-drug treatments. BRAF mutant individuals with advanced MM are better suited for a grouping therapy involving both BRAF inhibitor and MEK inhibitor.
CTLA-4 monoclonal antibody combined with PD-1 monoclonal antibody treatment
Due to distinct mechanisms and synergistic effects in T cell activation and tumor eradication, combining CTLA-4 and PD-1 monoclonal antibodies can exert a complementary and enhanced anti-tumor effect. KIRKWOODD et al. [54] highlighted the efficacy of combining epizumab and navumab. In a phase II clinical trial involving 142 metastatic MM patients, participants were randomly assigned to receive either the combined epizumab and navumab treatment or epizumab alone. The findings indicated clear benefits in the combined treatment group. Response rates were notably higher at 61%, compared to 11% in the other group. The complete remission proportion stood at 22% versus 0%. Additionally, the progression-free survival duration was significantly extended in the combined treatment group, reaching 8.9 months, compared to 4.7 months in the alternative group. Two-year survival rates also favored the combined treatment, with 64% compared to 54%. In the phase III clinical trial, patients undergoing combination therapy experienced an extended progression-free survival period of 11.5 months, compared to 6.9 months with navumab monotherapy and 2.9 months with epizumab monotherapy. Furthermore, the 3-year survival rates were notably higher at 58% for combination therapy, 52% for navumab monotherapy, and 34% for epizumab monotherapy. The occurrence of status three/four side effects remained consistent across the three groups, registering at 59%, 21%, and 28%, respectively [55]. Combining CTLA-4 monoclonal antibody with PD-1 monoclonal antibody offers substantial benefits, though it often comes with an elevated incidence of adverse events. There should be more studies involving the safety of the combination of drugs to improve this defect. Consider the synergy of CTLA-4 monoclonal antibody and PD-1 monoclonal antibody when paired with tumor-infiltrating lymphocytes or hereditarily adapted T cells. This combination induces targeted anti-tumor immune responses, consequently lowering the likelihood of immune-related adverse events [56].
Targeted therapy combined with immunotherapy
Currently, the primary therapeutic avenues for MM include targeting and immunotherapy. However, their mechanisms diverge significantly: the former exhibits a high efficacy and swift curative impact but is susceptible to drug resistance and characterized by a brief effective duration. In contrast, the latter approach often yields enduring effects, yet it predominantly involves delayed reactions and offers restricted benefits. Currently, numerous studies validate that inhibitors targeting the MAPK signaling pathway can enhance the release of tumor antigens. This process facilitates T cell recognition of tumor antigens, promotes the differentiation of T cell immunity towards TH1 reactions, and encourages the aggregation of cytotoxic T cells. Additionally, it activates NK cells, fostering their expansion, eliminates regulatory T cells, and diminishes the release of immunosuppressive cytokines (such as IL-1, IL-6, IL-8, IL-10, and vascular endothelial growth factor). However, it's noteworthy that these targeted drugs often induce the expression of inhibitory molecules like PD-1, PD-L1, TIM-3, and others on the cell surface as they exert their anti-tumor effects. Therefore, targeted drugs combined with immunotherapy (immune checkpoint inhibitors, cytokine therapy, adoptive cell immunotherapy, etc.) are likely to produce synergistic sensitization, play an early and strong anti-tumor effect, and obtain better clinical efficacy, which should be a reliable choice for late MM treatment in the near future. Relevant experiments have proved that BRAF/MEK inhibitor combined with CTLA-4/PD-1 monoclonal antibody has better efficacy than single targeted or immunotherapy [57].
Other combined treatment
According to early research, MM has low sensitivity to traditional radiotherapy and chemotherapy and poor efficacy, but both of them have synergistic anti-tumor effect when combined with targeted drugs or immunotherapy, which also adds hope to the treatment of MM patients [56]. MAPK signal pathway is closely related to the radio-sensitivity of tumor cells. At present, studies have confirmed that drug inhibition of MAPK pathway signal can improve the vulnerability of NRAS mutant MM cells to ionizing radiation; In preclinical studies, it was found that MEK inhibitor combined with radiotherapy can inhibit the growth of MM in animals and is well tolerated [58]. Therefore, MAPK signal pathway inhibitor combined with radiotherapy should significantly improve clinical benefits. MM is prone to brain metastasis, and 6.7% of newly diagnosed patients have brain metastasis. In the progression of the disease, approximately half of stage IV patients will experience brain metastasis, with a median overall survival time (mOS) ranging from 17 to 22 months. Currently, research indicates that combining immunotherapy with radiotherapy extends the survival duration of MM patients with brain metastasis. Moreover, administering radiotherapy before or concurrently with immunotherapy can prolong the interval until local recurrence occurs. [59]. Therefore, radiotherapy combined with targeted and/or immunotherapy can improve the local focus control rate and enhance the distant effect. To sum up, targeted drugs and/or immunotherapy combined with radiotherapy and chemotherapy should be an important research direction in the treatment of advanced MM in China. In fact, immunotherapy for MM or targeted therapy for BRAF inhibitors and MEK inhibitors has its unique advantages, but we should also see its limitations. More and more evidence show that new therapeutic drugs can produce more specific response to MM cells and lower toxicity to organisms when used in MM treatment. These new methods have won an increasingly important position in different MM treatment schemes. So far, there is still no relevant clear guideline for the treatment of MM patients to show its efficacy. The future treatment direction and strategy of MM should be the common responsibility and mission of all participants in the multidisciplinary medical team.
Prevention
There are three categories of melanoma prevention strategies: primary, secondary, and tertiary. Melanoma incidence is decreased in known high-risk populations due to primary prevention. The best course of action for its prevention is to stay out of the sun as much as possible because this lowers UV light exposure. Limit sun exposure, covering all skin with clothing, including a wide-brimmed hat. Additional preventive measures involve regular sunscreen application and enhancing clothing's photoprotection by using detergent [60].
In young children, sunburn prevention is crucial [61]. Educate parents and the community about sun protection, self-skin examination, and factors contributing to skin cancer risks [62]. Individuals with personal or family histories of melanoma should adopt preventive measures to minimize sun exposure. Cancer Council Victoria in Australia has been dedicated to this group for over two decades, implementing sun protection initiatives. Their educational efforts have led to a significant reduction in sun exposure and risky behaviors among at-risk individuals in their community [63]. Increased skill in identifying and treating early-stage melanoma is the secondary prevention of melanoma. Men aged 50 and above, individuals with giant congenital nevi, xeroderma pigmentosum, immunosuppression, abnormal nevi, familial atypical multiple mole and melanoma syndrome, and those with a family history of melanoma should undergo comprehensive initial and subsequent skin examinations by a healthcare professional. As part of a routine primary care medical evaluation, a dermatologist should thoroughly examine to screen for melanoma and treat any other skin issues. The incidence of melanoma diagnosis is rising due to continuous technological improvement [64]. Tertiary melanoma prevention arises from advances in therapy that extend the survival time of individuals with advanced illnesses. Early skin cancer identification results in reduced morbidity and mortality in the short and long term. Those who had their melanoma removed early had a higher survival rate. Scotland’s death rate has reduced as public information about melanoma prevention is becoming increasingly widespread in many nations. The sharp death rate has also decreased in older males with more extensive primary tumors. The reduction has been particularly noticeable in younger women. Treating tumors in their early stages reduces mortality and morbidity rates, according to early-stage detection programs [65,66]. Regular application of sunscreen decelerates the advancement of existing actinic or solar keratoses and hinders the formation of new ones in individuals. The prevalence of skin cancer in newborns with xeroderma pigmentosum has decreased due to educational campaigns urging people to limit their sun exposure [65].
Figures & Tables
Skin malignant melanoma stems from the malignancy of melanocytes, and its global incidence is rapidly increasing, presenting challenges for public health. Surgery is the first choice for the treatment of non-metastatic MM. However, considering the anatomical location, the number of lesions and the rate of recurrence after surgery, surgery is not suitable for all patients with MM. The development of new drugs for selective targeting and immunotherapy has improved the response rate, and immunization and targeted therapy are effective strategies for treating MM. There are many risk factors affecting the occurrence of skin melanoma, among which ultraviolet rays are the main factor causing skin melanoma. The hazard of melanoma to the general public's health is reduced by taking the proper preventative measures such as avoiding long-term sunlight exposure will help prevent the occurrence of skin melanoma. Appropriate preventive measures and treatment can help to improve the survival period of skin melanoma patients. Nevertheless, to enhance skin melanoma treatment and elevate patients' quality of life, additional research in related fields remains imperative.
Conflict of Interest
The authors declare no conflict of interest.
Honggang Yu and Rizwan Ali initiated the project. Honggang Yu, Rizwan Ali, Lei Rui, and Jinghong Xu made equal contributions to writing and editing the manuscript. Rizwan Ali oversaw the project and offered guidance. All authors have reviewed and consented to the publication of the final manuscript version.
![]() References
References
- Bloomston M, Frankel WL, Petrocca F, Volinia S, Alder H, et al. MicroRNA expression patterns to differentiate pancreatic adenocarcinoma from normal pancreas and chronic pancreatitis. The Journal of American Medical Association, (2007); 297 171901-1908.
- Jemal A, Devesa SS, Hartge P, Tucker MA. Recent trends in cutaneous melanoma incidence among whites in the United States. Journal of the National Cancer Institute, (2001); 93(9): 678-683.
- American Cancer Society (2020).Key statistics for melanoma skin cancer[EB/OL].[2021-09- 21 ]https://www.cancer.org/cancer/melano- m a-s k i n-c a n c e r/a b o u t/k e y-s t a t i s t i c s .h t m l.
- Ernst M, Giubellino A. The Current State of Treatment and Future Directions in Cutaneous Malignant Melanoma. Biomedicines, (2022); 10(4).
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. A Cancer Journal of Clinicians, (2021); 71(3): 209-249.
- Balch CM. Cutaneous melanoma: prognosis and treatment results worldwide. Seminars in Surgical Oncology, (1992); 8(6): 400-414.
- Cascinelli N, Zurrida S, Galimberti V, Bartoli C, Bufalino R, et al. Acral lentiginous melanoma. A histological type without prognostic significance. The Journal of Dermatologic Surgery and Oncology, (1994); 20(12): 817-822.
- Chang AE, Karnell LH, Menck HR. The National Cancer Data Base report on cutaneous and noncutaneous melanoma: a summary of 84,836 cases from the past decade. The American College of Surgeons Commission on Cancer and the American Cancer Society. Cancer, (1998); 83(8): 1664-1678.
- Ahmed B, Qadir MI, Ghafoor S. Malignant Melanoma: Skin Cancer-Diagnosis, Prevention, and Treatment. Critical reviews in eukaryotic gene expression, (2020); 30(4): 291-297.
- Edwards BK, Howe HL, Ries LA, Thun MJ, Rosenberg HM, et al. Annual report to the nation on the status of cancer, 1973-1999, featuring implications of age and aging on U.S. cancer burden. Cancer, (2002); 94(10): 2766-2792.
- Elwood JM, Gallagher RP. Site distribution of malignant melanoma. Canadian Medical Association Journal, (1983); 128(12): 1400-1404.
- Read RL, Haydu L, Saw RP, Quinn MJ, Shannon K, et al. In-transit melanoma metastases: incidence, prognosis, and the role of lymphadenectomy. Annals of Surgical Oncology, (2015); 22(2): 475-481.
- Tuli HS, Sak K, Iqubal A, Choudhary R, Adhikary S, et al. Recent Advances in Immunotherapy for the Treatment of Malignant Melanoma. Current Pharmaceutical Design, (2022); 28(29): 2363-2374.
- Long GV, Swetter SM, Menzies AM, Gershenwald JE, Scolyer RA. Cutaneous melanoma. Lancet, (2023); 402(10400): 485-502.
- Uhara H. Recent advances in therapeutic strategies for unresectable or metastatic melanoma and real-world data in Japan. International Journal of Clinical Oncology, (2019); 24(12): 1508-1514.
- Livingstone A, Agarwal A, Stockler MR, Menzies AM, Howard K, et al. Preferences for Immunotherapy in Melanoma: A Systematic Review. Annals of Surgical Oncology, (2020); 27(2): 571-584.
- Haanen JB. Immunotherapy of melanoma. European Journal of Cancer Supplements, (2013); 11(2): 97-105.
- Zappasodi R, Sirard C, Li Y, Budhu S, Abu-Akeel M, et al. Rational design of anti-GITR-based combination immunotherapy. Nature Medicine, (2019); 25(5): 759-766.
- Liu BL, Robinson M, Han ZQ, Branston RH, English C, et al. ICP34.5 deleted herpes simplex virus with enhanced oncolytic, immune stimulating, and anti-tumour properties. Gene Therapy, (2003); 10(4): 292-303.
- MacKie RM, Stewart B, Brown SM. Intralesional injection of herpes simplex virus 1716 in metastatic melanoma. Lancet, (2001); 357(9255): 525-526.
- Johnson DB, Puzanov I, Kelley MC. Talimogene laherparepvec (T-VEC) for the treatment of advanced melanoma. Immunotherapy, (2015); 7(6): 611-619.
- Senzer NN, Kaufman HL, Amatruda T, Nemunaitis M, Reid T, et al. Phase II clinical trial of a granulocyte-macrophage colony-stimulating factor-encoding, second-generation oncolytic herpesvirus in patients with unresectable metastatic melanoma. Journal of Clinical Oncology, (2009); 27(34): 5763-5771.
- Andtbacka RHI, Collichio F, Harrington KJ, Middleton MR, Downey G, et al. Final analyses of OPTiM: a randomized phase III trial of talimogene laherparepvec versus granulocyte-macrophage colony-stimulating factor in unresectable stage III-IV melanoma. Journal of Immunotherapy of Cancer, (2019); 7(1): 145.
- Mancuso P, Tricarico R, Bhattacharjee V, Cosentino L, Kadariya Y, et al. Thymine DNA glycosylase as a novel target for melanoma. Oncogene, (2019); 38(19): 3710-3728.
- Lugowska I, Teterycz P, Rutkowski P. Immunotherapy of melanoma. Contemporary Oncology (Pozn), (2018); 22(1a): 61-67.
- Hunder NN, Wallen H, Cao J, Hendricks DW, Reilly JZ, et al. Treatment of metastatic melanoma with autologous CD4+ T cells against NY-ESO-1. New England Journal of Medicine, (2008); 358(25): 2698-2703.
- Innamarato P, Kodumudi K, Asby S, Schachner B, Hall M, et al. Reactive Myelopoiesis Triggered by Lymphodepleting Chemotherapy Limits the Efficacy of Adoptive T Cell Therapy. Molecular Therapy, (2020); 28(10): 2252-2270.
- Villani A, Scalvenzi M, Fabbrocini G, Ocampo-Candiani J, Ocampo-Garza SS. Looking into a Better Future: Novel Therapies for Metastatic Melanoma. Dermatology and Therapy (Heidelb), (2021); 11(3): 751-767.
- Shi H, Lan J, Yang J. Mechanisms of Resistance to Checkpoint Blockade Therapy. Advances in Experimental Medicine and Biology, (2020); 124883-117.
- Buchbinder EI, Hodi FS. Melanoma in 2015: Immune-checkpoint blockade – durable cancer control. Nature Reviews Clinical Oncology, (2016); 13(2): 77-78.
- Khushalani NI, Diab A, Ascierto PA, Larkin J, Sandhu S, et al. Bempegaldesleukin plus nivolumab in untreated, unresectable or metastatic melanoma: Phase III PIVOT IO 001 study design. Future Oncology, (2020); 16(28): 2165-2175.
- Spitler LE, Boasberg P, O'Day S, Hamid O, Cruickshank S, et al. Phase II study of nab-paclitaxel and bevacizumab as first-line therapy for patients with unresectable stage III and IV melanoma. American Journal of Clinical Oncology, (2015); 38(1): 61-67.
- Corrie PG, Marshall A, Dunn JA, Middleton MR, Nathan PD, et al. Adjuvant bevacizumab in patients with melanoma at high risk of recurrence (AVAST-M): preplanned interim results from a multicentre, open-label, randomised controlled phase 3 study. Lancet Oncology, (2014); 15(6): 620-630.
- Weber J, Mandala M, Del Vecchio M, Gogas HJ, Arance AM, et al. Adjuvant Nivolumab versus Ipilimumab in Resected Stage III or IV Melanoma. New England Journal of Medicine, (2017); 377(19): 1824-1835.
- Zhang K, Guo L. MiR-767 promoted cell proliferation in human melanoma by suppressing CYLD expression. Gene, (2018); 641272-278.
- Rajkumar S, Berry D, Heney KA, Strong C, Ramsay L, et al. Melanomas with concurrent BRAF non-p.V600 and NF1 loss-of-function mutations are targetable by BRAF/MEK inhibitor combination therapy. Cell Reports, (2022); 39(1): 110634.
- Postow MA, Callahan MK, Wolchok JD. Immune Checkpoint Blockade in Cancer Therapy. Journal of Clinical Oncology, (2015); 33(17): 1974-1982.
- Haugh AM, Johnson DB. Management of V600E and V600K BRAF-Mutant Melanoma. Current Treatment Options in Oncology, (2019); 20(11): 81.
- Schadendorf D, Hodi FS, Robert C, Weber JS, Margolin K, et al. Pooled Analysis of Long-Term Survival Data From Phase II and Phase III Trials of Ipilimumab in Unresectable or Metastatic Melanoma. Journal of Clinical Oncology, (2015); 33(17): 1889-1894.
- Chiou VL, Burotto M. Pseudoprogression and Immune-Related Response in Solid Tumors. Journal of Clinical Oncology, (2015); 33(31): 3541-3543.
- Wilhelm SM, Carter C, Tang L, Wilkie D, McNabola A, et al. BAY 43-9006 exhibits broad spectrum oral antitumor activity and targets the RAF/MEK/ERK pathway and receptor tyrosine kinases involved in tumor progression and angiogenesis. Cancer Research, (2004); 64(19): 7099-7109.
- Flaherty KT, Lee SJ, Schuchter LM, Flaherty LE, Wright JJ, et al. Final results of E2603: A double-blind, randomized phase III trial comparing carboplatin (C)/paclitaxel (P) with or without sorafenib (S) in metastatic melanoma. Journal of Clinical Oncology, (2010); 28(15_suppl): 8511-8511.
- Ribas A, Kim KB, Schuchter LM, Gonzalez R, Pavlick AC, et al. BRIM-2: An open-label, multicenter phase II study of vemurafenib in previously treated patients with BRAF V600E mutation-positive metastatic melanoma. Journal of Clinical Oncology : official journal of the American Society of Clinical Oncology, (2011); 29 15_suppl8509.
- Chapman PB, Hauschild A, Robert C, Larkin JMG, Haanen JBAG, et al. Updated overall survival (OS) results for BRIM-3, a phase III randomized, open-label, multicenter trial comparing BRAF inhibitor vemurafenib (vem) with dacarbazine (DTIC) in previously untreated patients with BRAFV600E-mutated melanoma. Journal of Clinical Oncology, (2012); 30(15_suppl): 8502-8502.
- Kefford R, Arkenau H, Brown MP, Millward M, Infante JR, et al. Phase I/II study of GSK2118436, a selective inhibitor of oncogenic mutant BRAF kinase, in patients with metastatic melanoma and other solid tumors. Journal of Clinical Oncology, (2010); 28(15_suppl): 8503-8503.
- Ives NJ, Suciu S, Eggermont AMM, Kirkwood J, Lorigan P, et al. Adjuvant interferon-α for the treatment of high-risk melanoma: An individual patient data meta-analysis. European Journal of Cancer, (2017); 82171-183.
- Agarwala SS, Lee SJ, Yip W, Rao UN, Tarhini AA, et al. Phase III Randomized Study of 4 Weeks of High-Dose Interferon-α-2b in Stage T2bNO, T3a-bNO, T4a-bNO, and T1-4N1a-2a (microscopic) Melanoma: A Trial of the Eastern Cooperative Oncology Group-American College of Radiology Imaging Network Cancer Research Group (E1697). Journal of Clinical Oncology, (2017); 35(8): 885-892.
- Mohr P, Hauschild A, Trefzer U, Enk A, Tilgen W, et al. Intermittent High-Dose Intravenous Interferon Alfa-2b for Adjuvant Treatment of Stage III Melanoma: Final Analysis of a Randomized Phase III Dermatologic Cooperative Oncology Group Trial. Journal of Clinical Oncology, (2015); 33(34): 4077-4084.
- Eigentler TK, Gutzmer R, Hauschild A, Heinzerling L, Schadendorf D, et al. Adjuvant treatment with pegylated interferon α-2a versus low-dose interferon α-2a in patients with high-risk melanoma: a randomized phase III DeCOG trial. Annals of Oncology, (2016); 27(8): 1625-1632.
- Sosman JA, Kim KB, Schuchter L, Gonzalez R, Pavlick AC, et al. Survival in BRAF V600-mutant advanced melanoma treated with vemurafenib. New England Journal of Medicine, (2012); 366(8): 707-714.
- Trunzer K, Pavlick AC, Schuchter L, Gonzalez R, McArthur GA, et al. Pharmacodynamic Effects and Mechanisms of Resistance to Vemurafenib in Patients With Metastatic Melanoma. Journal of Clinical Oncology, (2013); 31(14): 1767-1774.
- Long GV, Weber JS, Infante JR, Kim KB, Daud A, et al. Overall Survival and Durable Responses in Patients With BRAF V600-Mutant Metastatic Melanoma Receiving Dabrafenib Combined With Trametinib. Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology, (2016); 34(8): 871-878.
- Robert C, Karaszewska B, Schachter J, Rutkowski P, Mackiewicz A, et al. Improved overall survival in melanoma with combined dabrafenib and trametinib. New England Journal of Medicine, (2015); 372(1): 30-39.
- Kirkwood J, Long G, Trefzer U, Davies M, Ascierto P, et al. BREAK-MB: A phase II study assessing overall intracranial response rate (OIRR) to dabrafenib (GSK2118436) in patients (pts) with BRAF V600E/k mutation-positive melanoma with brain metastases (mets). Journal of Clinical Oncology, (2012); 308501-8501.
- Wolchok JD, Chiarion-Sileni V, Gonzalez R, Rutkowski P, Grob JJ, et al. Overall Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma. New England Journal of Medicine, (2017); 377(14): 1345-1356.
- Fusi A, Dalgleish A. The importance for immunoregulation for long-term cancer control. Future Oncology, (2017); 13(18): 1619-1632.
- 任宇, 刘宝瑞, 邹征云. 晚期恶性黑色素瘤的靶向及免疫治疗研究进展. 现代肿瘤医学, (2018); 26(12): 1970-1974. Ren Yu, Liu Baorui, and Zou Zhengyun. "Research Progress on Targeted and Immunotherapy for Advanced Malignant Melanoma." Modern Oncology, 2018; 26(12): 1970-1974.
- Schick U, Kyula J, Barker H, Patel R, Zaidi S, et al. Trametinib radiosensitises RAS- and BRAF-mutated melanoma by perturbing cell cycle and inducing senescence. Radiotherapy and oncology : Journal of the European Society for Therapeutic Radiology and Oncology, (2015); 117.
- Cohen-Inbar O. PS1 – 140 The Effect of Timing of Stereotactic Radiosurgery Treatment of Melanoma Brain Metastases Treated with Ipilimumab. Canadian Journal of Neurological Sciences, (2016); 43(S4): S6-S7.
- Markovic SN, Erickson LA, Rao RD, Weenig RH, Pockaj BA, et al. Malignant melanoma in the 21st century, part 1: epidemiology, risk factors, screening, prevention, and diagnosis. Mayo Clinic Proceedings, (2007); 82(3): 364-380.
- Kaskel P, Sander S, Kron M, Kind P, Peter RU, et al. Outdoor activities in childhood: a protective factor for cutaneous melanoma? Results of a case-control study in 271 matched pairs. British Journal of Dermatology, (2001); 145(4): 602-609.
- Grob JJ, Guglielmina C, Gouvernet J, Zarour H, Noé C, et al. Study of sunbathing habits in children and adolescents: application to the prevention of melanoma. Dermatology, (1993); 186(2): 94-98.
- Montague M, Borland R, Sinclair C. Slip! Slop! Slap! and SunSmart, 1980-2000: Skin cancer control and 20 years of population-based campaigning. Health Education and Behavior, (2001); 28(3): 290-305.
- Aitken JF, Janda M, Elwood M, Youl PH, Ring IT, et al. Clinical outcomes from skin screening clinics within a community-based melanoma screening program. Journal of American Academy of Dermatology, (2006); 54(1): 105-114.
- Marks R. An overview of skin cancers. Incidence and causation. Cancer, (1995); 75(2 Suppl): 607-612.
- Qadir MI. Skin cancer: Etiology and management. Pakistan Journal of Pharmaceutical Sciences, (2016); 29(3): 999-1003
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0