

Short Communication
Diabetes and Hepatitis C: Two sides of a coin
Muhammad Atif1*, Sana Arshad2, Khursheed Javaid1, Maaz ul Hassan3, Fayyaz Ahmad1, Muhammad Imran4, Muhammad Imran5, Arshad Jamal1, Zareen Fatima6, Ahmed Bilal Waqar7
Adv. life sci., vol. 4, no. 3, pp. 72-76, May 2017
*- Corresponding Author: Muhammad Atif (Email: aatif03@gmail.com)
Authors' Affiliations
2- UIMLT, Faculty of Allied Health Sciences, University of Lahore, Lahore – Pakistan
3- Surgical Unit III, Shalamar Medical College, Lahore – Pakistan
4- DDNS, Faculty of Health and Allied Sciences, Imperial College of Business Studies, Lahore – Pakistan
5- Department of Microbiology, University of Health Sciences, Lahore – Pakistan
6- DRSMI, Faculty of Health and Allied Sciences, Imperial College of Business Studies, Lahore – Pakistan
7- IPGMI, Faculty of Health and Allied Sciences, Imperial College of Business Studies, Lahore – Pakistan
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Hepatitis C virus or HCV is a blood borne pathogen, transmitted primarily via blood, body secretions and by piercing through skin (percutaneous), veins and mucosal surfaces. Prevalence of HCV in Pakistan is 4.5-8%. The prevalence of HCV in diabetic patients is reported to be 14.9% in 2016. Different studies show different prevalence of Hepatitis C in local population of Pakistan. This study was designed to find out the prevalence of HCV in diabetic patients of different age groups and gender.
Methods: Blood samples from 259 diabetic patients were collected at Diabetes Testing and Screening Camp arranged by Akhuwat Health Services (AHS) at Township, Lahore. People of all age groups and gender were invited. Results were entered in MS Excel and analyzed on SPSS 19.
Results: Out of 259 patients, 53% were females while 47% were males. This study shows the prevalence of HCV in Diabetic Patients as 8%. It was observed in diabetic patients, that females and patients from age group 30-40 years had high prevalence of HCV.
Conclusion: The prevalence of Hepatitis C is high in the diabetic patients as compared to general population. HCV has a greater incidence in diabetic females of age group (30-40 years).
Key words: Hepatitis, Diabetes, Age, Gender
Introduction
Viral hepatitis is one of the most serious pandemic disease. Many viruses cause hepatitis, but only few of them are medically important, which include HCV, HBV, HAV, HEV and HDV [1-3]. Number of studies have been done to find out the prevalence of HCV in Pakistan and worldwide [4, 5]. To check the variations in prevalence of HCV in the world, countries are grouped into Global Burden of Disease regions. The highest prevalence of HCV is reported to be in Central/East Asia (3.8%) and North Africa/Middle East regions (3.6%) [6]. HCV is an emerging major health issue of developing countries, including Pakistan having a prevalence rate of 4.5% to 8% (second highest prevalence rate of hepatitis C among developing countries). Prevalence rate of HCV is as high as 25% in rural and underdeveloped peri-urban areas and 40% in small targeted groups including drug abusers, blood donors, chronic liver disease patients and healthcare professionals. However, literature is still not conclusive to portrait the real image due to its limitation on identifying the incidence in healthy individuals [4, 7, 8]. Recent studies show that there are 130-175 million people suffering from HCV out of which 350,000 die annually [6]. The prevalence of Hepatitis C in adult male of Punjab and Northern Pakistan is 4.5% and 4.0% respectively [9, 10]. The prevalence of Hepatitis C in Type 2 Diabetes Mellitus is 14.9% [11].
HCV is a small, enveloped single stranded RNA virus; two types of glycoproteins (E1 and E2) are present on its surface. E2 glycoprotein binds the host cell through the interaction with scavenger receptor class B type I (SR-B1) and CD81 thus, target the neutralizing antibodies [12-14]. HCV is a blood borne pathogen, transmitted primarily via blood, other body secretions and by piercing through skin (percutaneous), veins and mucosal surfaces [2,3,15]. The major modes of transmission of HCV are; through unsafe therapeutic injections usage, transfusion of blood and blood product, shaving with unsterilized instruments by barbers, tattooing, transmission from mother to child, unsafe sexual intercourse, hemodialysis, needle-stick injuries among health professionals, and poor personal hygiene habits [16-19].
Re-use of contaminated needles or surgical instruments and improper screening of blood are the major risk factors [15]. Low socioeconomic status and poor hygienic environment are considered to be other major factors of such high rate of HCV infection [20]. Approximately, 67% population in 148 countries are infected with HCV through injecting drugs [21]. Globally, reuse of unsterilized injections leads to approximately 2-5 million HCV infections, which lead to the high burden of morbidities and mortalities [22, 23]. HCV infection has serious sequel; it can lead to acute and chronic hepatitis, liver diseases, liver cirrhosis or hepato-cellular carcinoma (HCC). Acute Hepatitis C clears within 6 months in 20% cases and about 80% cases become chronic and may progress in chronic liver diseases [2, 7, 24].
The aim of this study was to find the prevalence of Hepatitis C in diabetic patients in different age groups and gender.
Methods
In this cross sectional study, blood samples from 259 diabetic patients were collected at Diabetes Testing and Screening Camp by Akhuwat Health Services (AHS) at Township, Lahore. People of all age groups and genders were invited. Blood was collected in evacuated tubes containing EDTA as an anti-coagulant. Tubes were centrifuged at 3400-4000 RPM for 5-10 minutes to collect plasma, which was stored at -2°C ice bags. Samples were taken to the laboratory, where HCV screening test was done on Immuno-chromatographic Kits of RapiCard™ InstaTest (Reference Number 118773-1-44) by Diagnostic Automation/Cortez Diagnostic Incorporation USA. Results of the laboratory tests were stored in Microsoft EXCEL and analyzed using the Statistical Package for Social Sciences (SPSS 19.0.verison).
Results
Distribution of Diabetic Patients
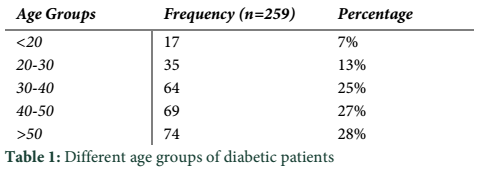
In this cross-sectional study, total 259 patients were screened. Out of 259 patients, 53% (138/259) were females while 47% (121/259) were males. Frequency of different age groups <20, 20-30, 30-40, 40-50 and >50 years were 7% (17/259), 13% (35/259), 25% (64/259), 27% (69/259) and 28% (74/259) respectively (Table 1).
Distribution of HCV Positive Diabetic Patients
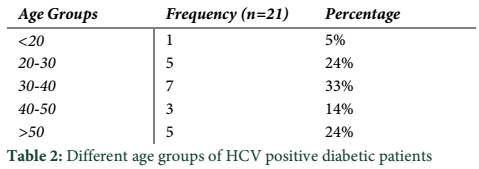
The prevalence of HCV in Diabetic Patients was 8% (21/259). Out of 21 HCV positive patients, 62% (13/21) were females while 38% (8/21) were males. The proportion of HCV positive patients on their age groups <20, 20-30, 30-40, 40-50 and >50 years were 5% (1/21), 24% (5/21), 33% (7/21), 14% (3/21) and 24% (5/21) (Table 2).
When the frequencies of age and gender of positive cases of HCV were checked, there were remarkable difference seen in both gender and age groups. Prevalence of HCV was significantly high in diabetic females (62%) as compared to diabetic male (38%). It was also observed in the results of this study that the prevalence of diabetes was high in 30-40 years age group i.e. 33% as shown in table 2.
Tables & Figures
Discussion
This study was conducted to evaluate the prevalence of Hepatitis C in diabetic patients of different age and gender. Current study estimates the prevalence of HCV as 8% in diabetic patients. Hussain et al, also reported a high prevalence (14.9%) of HCV in diabetic patients in 2016 [11]. Findings of other studies done in Pakistan, UK, USA also support result of current study [25-28]. L. K. Chen et al in 2005 reported that a prevalence of HCV in diabetic patients which he reasoned might be the complication of diabetic therapy [29]. Result of current study are comparable to the studies done in Saudi Arabia [30] and Greek [31] and in Islamabad [32], Multan [26], Jhelum [33], Faisalabad [34] and Wah Cantt [35].
Results of this study revealed that hepatitis C is highly prevalent in diabetic females as compared to diabetic males. In 2016, same results were reported in the study of Essa [30] and Kanwal [36]. There was no significant difference seen in the study of Jadoon and Ndako [26,37]. In contrary, Rehman et al in 2017 reported the highest prevalence of HCV in diabetic males [38].
The result showed that adults (30-40 years) have high frequency of HCV that was 33%. Same results were showed in the study of Rehman (2017) and Bostan (2016) [38, 39]. Ahmad et al in 2010 reported the same kind of results that frequency of HCV infection in people ≤ 40 years of age was higher than those people > 40 years of age in Lahore [40]. Results of this study are in conflict with the previous studies of N. Muhammad et al in 2005 which showed that prevalence of HCV in Pakistan is more frequent in > 50 years of age [41]. Previous studies showed that the prevalence of HCV was high in 45-55 years of age groups [37, 42]. This might be due to an early diagnosis and increasing awareness of HCV in urban areas of Pakistan [16]. N. H. Saleem et al in 2008 showed that the modes of transmission of HCV were more significantly linked with age groups however other risk factors like blood transfusion, dental surgery and road accidents equally distributed in all age groups [43].
The prevalence of Hepatitis C is high in the diabetic patients as compared to the general population of Lahore, Pakistan. Diabetic patients of age group (30-40) years have the highest risk for HCV. In diabetic patients gender is also a risk factor for the Hepatitis C. Further studies are needed to find out the basics behind these high prevalence.
Reference
- Shah U, Habib Z. Liver failure attributable to hepatitis A virus infection in a developing country. Pediatrics, (2000); 105(2): 436-438
- Ali SA, Donahue RMJ, Qureshi H, Vermund SH. Hepatitis B and hepatitis C in Pakistan: prevalence and risk factors. International Journal of Infectious Diseases, (2009); 13(1): 9-19.
- Bosan A, Qureshi H, Bile KM, Ahmad I, Hafiz R. A review of hepatitis viral infections in Pakistan. Journal of Pakistan Medical Association, (2010); 60(12): 1045-1058.
- Jiwani N. A Silent Storm: Hepatitis C in Pakistan. Journal of Pioneering Medical Sciences, (2011); 1(3): 89-91.
- Hoofnagle JH. Hepatitis C: the clinical spectrum of disease. Hepatology, (1997); 26(S3): 15-20.
- Mohamed AA, Elbedewy TA, El-Serafy M, El-Toukhy N, Ahmed W, et al. Hepatitis C virus: A global view. World Journal of Hepatology, (2015); 7(26): 2676-2680.
- World Health O (2013) WHO fact sheet 164-hepatitis C. WHO.
- Umer M, Iqbal M. Hepatitis C virus prevalence and genotype distribution in Pakistan: Comprehensive review of recent data. World Journal Of Gastroenterology, (2016); 22(4): 1684-1700.
- Simó R, Hernández C, Genescà J, Jardí R, Mesa J. High prevalence of hepatitis C virus infection in diabetic patients. Diabetes Care, (1996); 19(9): 998-1000.
- Khattak MF, Salamat N, Bhatti FA, Qureshi TZ. Seroprevalence of hepatitis B, C and HIV in blood donors in northern Pakistan. Journal Pakistan Medical Association, (2002); 52(9): 398-402.
- Hussain MZ, Afzal M, Sumreen, Kashif MA, Sher F, et al. The Frequency of Hepatitis C in the patients of Type II Diabetes Mellitus with good Glycemic control versus poor Glycemic control. Pakistan Armed Forces Medical Journal, (2016); 66: 72-75.
- Pileri P, Uematsu Y, Campagnoli S, Galli G, Falugi F, et al. Binding of hepatitis C virus to CD81. Science, (1998); 282(5390): 938-941
- Sautto G, Tarr AW, Mancini N, Clementi M. Structural and antigenic definition of hepatitis C virus E2 glycoprotein epitopes targeted by monoclonal antibodies. Clinical and Developmental Immunology, (2013); 2013: 1-12.
- Scarselli E, Ansuini H, Cerino R, Roccasecca RM, Acali S, et al. The human scavenger receptor class B type I is a novel candidate receptor for the hepatitis C virus. The EMBO Journal, (2002); 21(19): 5017-5025.
- Masood Z, Jawaid M, Khan RA, Rehman S. Screening for hepatitis B & C: a routine pre-operative investigation. Pakistan Journal of Medical Sciences, (2005); 21(4): 455-459.
- Ali M, Kanwal L, Tassaduqe K, Iqbal R. Prevalence of hepatitis C virus (HCV) in relation to its promotive factors among human urban population of Multan, Pakistan. European Journal of General Medicine, (2009); 6(2): 94-98.
- Haley RW, Fischer RP. Commercial tattooing as a potentially important source of hepatitis C infection: clinical epidemiology of 626 consecutive patients unaware of their hepatitis C serologic status. Medicine, (2001); 80(2): 134-151
- Lauer GM, Walker BD. Hepatitis C virus infection. New England Journal of Medicine, (2001); 345(1): 41-52.
- Raja NS, Janjua KA. Epidemiology of hepatitis C virus infection in Pakistan. Journal of Microbiology Immunology and Infection, (2008); 41(1): 1684-1182.
- Ahmad J, Taj AS, Rahim A, Shah A, Rehman M. Frequency of Hepatitis B and Hepatitis C in healthy blood donors of NWFP: a single center experience. Journal of Postgraduate Medical Institute (Peshawar-Pakistan), (2004); 18(3). 343-352.
- Tillmann HL, Thursz M. Hepatitis C Virus Infection—Its Role in Pathogenesis. Journal of Infectious Diseases, (2007); 195(2): 168-170.
- Kane A, Lloyd J, Zaffran M, Simonsen L, Kane M. Transmission of hepatitis B, hepatitis C and human immunodeficiency viruses through unsafe injections in the developing world: model-based regional estimates. Bulletin of the World Health Organization, (1999); 77(10): 801-807.
- Krajden M, McNabb G, Petric M. The laboratory diagnosis of hepatitis B virus. Canadian Journal of Infectious Diseases and Medical Microbiology, (2005); 16(2): 65-72
- Bari A, Akhtar S, Rahbar MH, Luby SP. Risk factors for hepatitis C virus infection in male adults in Rawalpindi–Islamabad, Pakistan. Tropical Medicine & International Health, (2001); 6(9): 732-738.
- Ali SS, Ali IS, Aamir AH, Jadoon Z, Inayatullah S. Frequency of hepatitis C infection in diabetic patients. Journal Ayub Medical College Abbottabad, (2007); 19(1): 46-49.
- Jadoon NA, Shahzad MA, Yaqoob R, Hussain M, Ali N. Seroprevalence of hepatitis C in type 2 diabetes: evidence for a positive association. Virology Journal, (2010); 7(1): 304.
- Gray H, Wreghitt T, Stratton IM, Alexander GJM, Turner RC, et al. High Prevalence of Hepatitis C Infection in Afro‐Caribbean Patients with Type 2 Diabetes and Abnormal Liver Function Tests. Diabetic Medicine, (1995); 12(3): 244-249.
- Rudoni S, Petit JM, Bour JB, Aho LS, Castaneda A, et al. HCV infection and diabetes mellitus: influence of the use of finger stick devices onnosocomial transmission. Diabetes and Metabolism, (1999); 25(6): 502-505.
- Chen LK, Chou YC, Tsai ST, Hwang SJ, Lee SD. Hepatitis C virus infection‐related Type 1 diabetes mellitus. Diabetic Medicine, (2005); 22(3): 340-343.
- Ba-Essa EM, Mobarak EI, Al-Daghri NM. Hepatitis C virus infection among patients with diabetes mellitus in Dammam, Saudi Arabia. BMC Health Services Research, (2016); 16(1): 313.
- Sotiropoulos A, Peppas TA, Skliros E, Apostolou O, Kotsini V, et al. Low prevalence of hepatitis C virus infection in Greek diabetic patients. Diabetic Medicine, (1999); 16(3): 250-252.
- Khokhar N. Association of chronic hepatitis C virus infection and diabetes mellitus. Pakistan Journal of Medical Research, (2002); 41(4): 155-158.
- Shahid MA. Diabetes Mellitus: Prevalence in patients of hepatitis C. Professional Medical Journal, (2012); 19(1): 68-72.
- Muhammad D, Amin K, Anjum A, Javed M. Chronic Hepatitis C Virus Infection; Association With Type 2 Diabetes Mellitus. Professional Medical Journal, (2010); 17(4): 557-562.
- Mansoor S, Bhutta S. Prevalence of Diabetes in Patients with HCV Hepatitis and Cirrhosis. Annals of Pakistan Institute of Medical Sciences, (2013); 9(4): 172-175.
- Kanwal N, Nasir B, Abrar MA, Kaukab I, Nawaz A, et al. Prevalence Of Hepatitis C In Diabetic Patients: A Prospective Study. Acta Poloniae Pharmaceutica, (2016); 73(3): 771-775.
- Ndako JA, Echeonwu GO, Shidali NN, Bichi IA, Paul GA, et al. Occurrence of hepatitis C virus infection in type 2 diabetic patients attending Plateau state specialist hospital Jos Nigeria. Virology Journal, (2009); 6(1): 98.
- Rehman GU, Ali M, Shah F, Iqbal A, Ahmad A, et al. Prevalence of Diabetes Type 2 in Hepatitis C Infected Patients in KPK, Pakistan. BioMed Research International, (2017); 2017: 2416281.
- Bostan N, Naeem M, Afzal MS, Shah ZH, Mustafa I, et al. Sero-prevalence of Hepatitis B and C Virus from rural areas of northern Punjab (Sargodha District), Pakistan. Tropical Biomedicine, (2016); 33(4): 599-607.
- Ahmad W, Ijaz B, Javed FT, Jahan S, Shahid I, et al. HCV genotype distribution and possible transmission risks in Lahore, Pakistan. World Journal of Gastroenterology, (2010); 16(34): 4321-4328.
- Muhammad N, Jan MA. Frequency of hepatitis" C" in Buner, NWFP. Journal of the College of Physicians and Surgeons–Pakistan: JCPSP, (2005); 15(1): 11-14.
- Mehta SH, Brancati FL, Strathdee SA, Pankow JS, Netski D, et al. Hepatitis C virus infection and incident type 2 diabetes. Hepatology, (2003); 38(1): 50-56.
- Saleem NH, Adrien A, Razaque A. Risky sexual behavior, knowledge of sexually transmitted infections and treatment utilization among a vulnerable population in Rawalpindi, Pakistan. Southeast Asian Journal of Tropical Medicine and Public Health, (2008); 39(4): 642-648.


