

Full Length Research Article
Prevalence of Hepatitis C and associated risk factors among pregnant women of district Nowshera, Khyber Pakhtunkhwa
Zobia Afsheen1*, Bashir Ahmad2, Huang Linfang3
Adv. life sci., vol. 5, no. 4, pp. 166-170, August 2018
*- Corresponding Author: Zobia Afsheen (Email: zobia.afsheen@abasyn.edu.pk)
Authors' Affiliations
2- Center of Biotechnology and Microbiology, University of Peshawar, Pakistan
3- Institute of Medicinal Plant Development (IMPLAD), Peking Union Medical College, Chinese Academy of Medical Sciences (CAMS), China
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: The epidemiological study of Hepatitis caused by Hepatitis C viruses during pregnancy is absolutely necessary for program managers and health planners. Currently, enough data exist regarding viral hepatitis among pregnant women in various districts of KP, Pakistan, however, proper published data from district Nowshera is not available. The study was aimed at determining the prevalence of hepatitis C infection along with its associated risk factors among pregnant women who attended the antenatal clinics at district Nowshera, KP.
Methods: One hundred and fifty (150) blood samples were obtained from pregnant women attending antenatal centers at district headquarter hospital Nowshera. Rapid immune-chromatographic technique (ICT) was used for detection of antibodies against HCV. Further confirmation of antibodies was done using Enzyme Linked Immunosorbent Assay (ELISA) followed by Reverse-transcription polymerase chain reaction (RT-PCR) for detection of HCV-RNA.
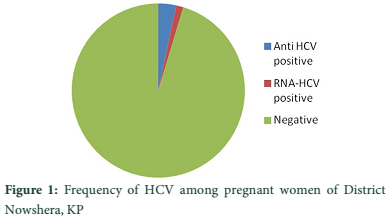
Results: Among 150 pregnant women, 7 (4.66%) were positive for HCV of which 5 (3.33%) were found positive for Anti-HCV antibodies while 2(1.33%) showed positivity for HCV-RNA. A significant association of age (x2 = 9.345, df = 3, P = 0.025), Gravidity (x2 = 9.15, df = 2, P = 0.010), education (x2 = 48.00, df = 5, P = 0.000), and Blood Transfusion (x2 = 4.629, df = 1, P = 0.031) was found with prevalence of HCV.
Conclusion: The study revealed 4.66% HCV prevalence among pregnant women of district Nowshera. The age, gravidity, and blood transfusion were the risk factors found significantly associated with HCV positivity in pregnant women. Additionally, the educational level of these women was also linked with the viral infection.
Keywords: Hepatitis C virus, Pregnancy, Risk factor association, Nowshera
Introduction![]()
Hepatitis C viral infection is a worldwide health problem. According to an estimate by World Health Organization (WHO), 3% of the world's populations have chronic HCV infections, of which the highest HCV prevalence rate is reported from Africa [1, 2]. The most efficient mode of HCV transmission is direct percutaneous inoculation. Many studies have demonstrated that household, occupational, sexual and vertical transmissions of HCV are also important as contributing factors [3]. It has been estimated that more than 170 million chronic HCV carriers across the world having risks of developing hepatic(liver) cancer, liver cirrhosis or both [4]. It is thought of as an important cause of jaundice and acute hepatitis in pregnancy and other complications [5].
Primarily, HCV spreads by direct contact with human blood [6]. However, during pregnancy, HCV was found to be associated with a high rate of vertical transmission, high risks of maternal complications, neonatal and fetal hepatitis. It has also been reported as major cause of maternal mortality [7-10].
Screening of blood products for hepatitis C viral antibodies has reduced such mode of HCV acquisition and leave the vertical transmission as a predominant mode of infection in infants. It is worthy to note that women who have caesarean section, vaginal birth or any other gynecological procedure which require blood transfusion are always have risk of hepatitis C. Vertical transmission of hepatitis C virus might occur during lactation, at conception, perinatally or in utero but its actual mechanism of transmission, including timing is still undiscovered [11]. In developed countries, the most common cause of HCV infection in children is maternal-child transmission (MCT) with an estimated rate of 5% transmission [12].
Currently, no vaccine is available to prevent hepatitis viral infection. Treatment for chronic hepatitis C is too costly for a person in developing countries. From the global perspective, efforts should be made to reduce risk of HCV transmission from nosocomial (hospital acquired) exposure, blood transfusion and unsafe injections practices [1]. Given that childbearing women have high risk of transmitting HCV infection, there is dire need to identify HCV carriers among women in the district under study. This study therefore is aimed at the detection of pregnant women with HCV infection, increasing awareness about viral hepatitis and aiding health care providers for the management of infected individuals. It is also aimed at preventing emanating complications of HCV and to diminish its attendant socio-economic load in the study area assuming its presence is established.
Methods![]()
Study area: The study was hospital based and the sampling was carried out at district headquarter hospital Nowshera. Due ethical clearance was taken for the study.
Study population: One hundred and fifty (150) blood samples were obtained from women attending antenatal clinics at district headquarter hospital Nowshera. Informed consent was taken from every participant. A structured questionnaire was designed to obtain their socio-demographic predispositions and risk factors (Table1) that exposed individuals to HCV infection.
Collection of blood sample and processing: 10ml of blood was obtained from the arm by venepuncture after disinfection with 70% alcohol. Five ml of the sample was placed in sterile labelled test tubes and allowed to clot. The sera were separated out into pre-labelled vials and were stored at -20oC until tested for detection of antibodies while rest of 5ml of samples were used for the detection of HCV-RNA.
Screening for HCV antibodies: Rapid immuno-chromatographic technique (ICT) was used for the detection of HCV-antibodies. Further confirmation of antibodies was done using ELISA. Manufacturer’s instructions were strictly adhered to IVD-REF E0320 micro-plate ELISA.
Screening for HCV-RNA: Reverse-transcription polymerase chain reaction (RT-PCR) was used to test the blood samples for the presence of HCV-RNA using Sacace Kit HCV Real-TM Qual.
Statistical analysis: The data obtained were entered in computer and checked twice before analysis using SPSS 20.0 version. The means and percentages were calculated. To compare the means and percentages between the sero-positive and sero-negative (HCV), Chi-square test was used. The age, gravidity, education and some other possible risk factors were taken as independent variable. The p-values less than 0.05 were considered as significant.
Results![]()
Among 150 pregnant women, 7 (4.66%) were positive for HCV of which 5 (3.33%) were found positive for Anti-HCV while 2 (1.33%) were positive for HCV-RNA.
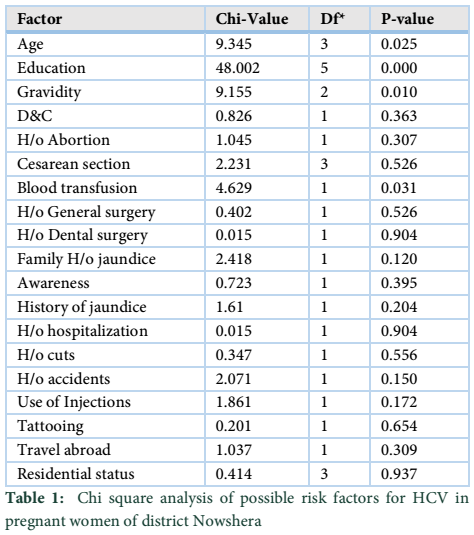
To test the association between different risk factors and prevalence of HCV, Chi-square test of association was utilized. Several different factors were tested for their association with HCV. A total of 19 different factors namely: age, education, gravidity, dilation and curettage (D&C), history of abortion, cesarean section, blood transfusion, history of general surgery, tooth surgery, jaundice, accidents, cuts, use of injections, tattooing, family history of liver disease/jaundice, traveling abroad, residential status and awareness were tested for association with prevalence of HCV. The results obtained were of mixed type, 15 factors namely Dilation and curettage (D&C), history of abortion, cesarean section, history of general surgery, tooth surgery, jaundice, accidents, cuts, use of injections, tattooing, family history of liver disease/jaundice, traveling abroad, residential status and awareness were found to have no significant relationship with prevalence of HCV. However, the results reveal a significant association of age (x2 = 9.345, DF = 3, P = 0.025), Gravidity (x2 = 9.15, DF = 2, P = 0.010), education (x2 = 48.00, DF = 5, P = 0.000), and blood transfusion (x2 = 4.629, DF = 1, P = 0.031) with prevalence of HCV (Table1).
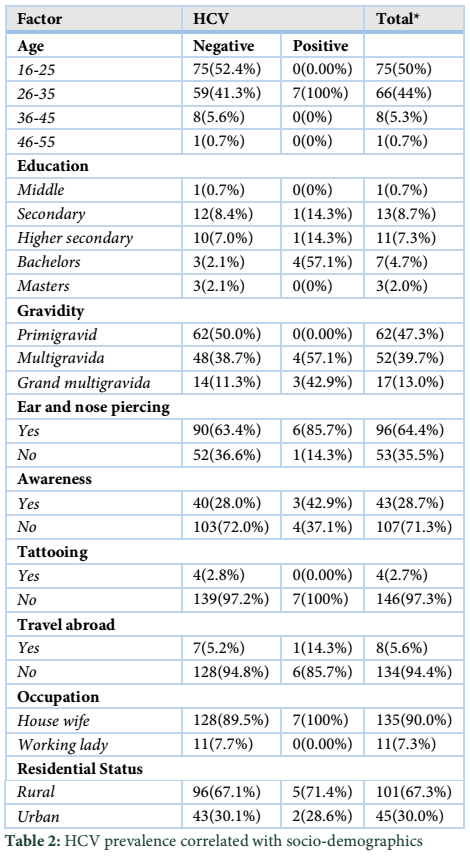
HCV positivity was confined to women of age group 26-35 years. Statistically, there exist a significant difference in association between seroprevalence of HCV and age (P = 0.025).
The seroprevalence of HCV with respect to demographics indicated that except for age, gravidity, education and blood transfusion rest of the factors did not play a main role in disease contraction.
Tables & Figures
Discussion![]()
This study is the first document being published on prevalence of HCV among pregnant women of district Nowshera, KP. Different epidemiologic studies have shown HCV seroprevalence in Pakistan with a range of 0.7% to 20% [13]. In our study, 4.66% of the pregnant women were found positive for HCV which is comparable with the findings of other such epidemiologic study [14].
Our finding of 4.66% prevalence has vital health implications for the large number of pregnant women and their families who dwell in our location of study. This is because the majority of the infected women were ignorant of HCV infection and were not aware of their infection status as they were asymptomatic. This imply that there is substantial potential for transmission of HCV infection to other people in their surrounding especially to fetuses. Our finding is parallel to a report from Mardan, which showed 4.34% prevalence of HCV [15] and that of 5.31% in a study at Islamabad [16].
The seroprevalence of HCV in our study was low when compared with that described previously in a study conducted in 2002 in Sindh, Pakistan which showed high HCV prevalence rate of 9% [17]. These pragmatic differences may be attributed to the degree of exposure to risk factors in our study populations as we found out that demographic variables considered in study had no statistical significance with HCV seropositivity.
Studies by Khan in 2004 and Muhammad 2004 has showed history of reused syringes, dental procedure, surgical operation, blood transfusion and tattooing as significant risk [18,19]. Similarly, study by Batash also showed that intramuscular injections and blood transfusions were significantly associated with HCV seropositivity [20]. Our results again reiterate their findings as blood transfusion (x2 = 4.629, DF = 1, P = .031) and Gravidity (x2 = 9.15, DF = 2, P = .010) to be significantly associated with HCV.
Similarly, studies by Cacoub found transfusion of blood products (P < 0.0001), and dental treatment (P < 0.0001) and Nafeh showed previous blood transfusions and sexual contacts with intravenous drug user [21, 22] as factors associated with HCV. Delage also showed intravenous drug use (P value 0.001) and blood transfusion (P value 0.01) to be statistically significant factors similar to our study [23].
As far the age groups screened, the highest prevalence of 100% was recorded among pregnant women of age group 26-35 years. This result agrees with the result in other studies which showed increase in HCV seroprevalence with increase in age [24]. Interestingly, statistical analysis showed a significant association between the age and HCV positivity (P = 0.025).
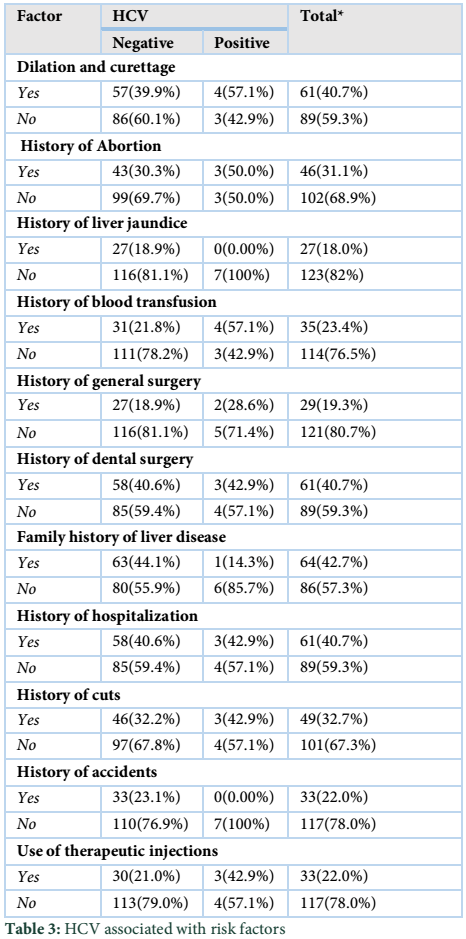
This was also interesting to note that in our study many factors like dilation and curettage (D&C), history of abortion, cesarean section, history of general surgery, tooth surgery, jaundice, accidents, cuts, use of injections, tattooing, family history of liver disease/jaundice, traveling abroad, residential status and awareness were found to have no significant relationship with prevalence of HCV. The possible justification was female sample population selected. As tattooing and traveling to abroad is not common in females of our society.
The study revealed a high rate of 4.66% HCV prevalence among pregnant women of district Nowshera. The age, gravidity, and blood transfusion were the risk factors found significantly associated with HCV positivity in pregnant women. Additionally, the educational level of these women was also linked with the infection.
Conflict of interest
Authors declare that there is no conflict of interest for publishing this study.
References![]()
- Lavanchy D. Global surveillance and control of hepatitis C. Report of a WHO Consultation organized in collaboration with the Viral Hepatitis Prevention Board, Antwerp, Belgium. Journal of viral hepatitis, (1999); 6(1): 35-47.
- Madhava V, Burgess C, Drucker E. Epidemiology of chronic hepatitis C virus infection in sub-Saharan Africa. The Lancet infectious diseases, (2002); 2(5): 293-302.
- Memon MI, Memon MA. Hepatitis C: an epidemiological review. Journal of viral hepatitis, (2002); 9(2): 84-100.
- Nwankiti OO, Ejekwolu AJ, Ndako AJ, Chollom S, Samuel E. A survey for antibodies to hepatitis C virus among women of childbearing Age. Nature and Science, (2012); 10(9): 148-152.
- Ojule AC, Akani CI, Opurum HC. Seroprevalence of hepatitis C antibodies in pregnant women in Port Harcourt, Nigeria. Port Harcourt Medical Journal, (2008); 3(1): 55 – 61.
- Villano SA, Vlahov D, Nelson KE, Cohn S, Thomas DL. Persistence of viremia and the importance of long‐term follow‐up after acute hepatitis C infection. Hepatology, (1999); 29(3): 908-914.
- Elinav E, Ben–Dov IZ, Shapira Y, Daudi N, Adler R, Shouval D, Ackerman Z. Acute hepatitis A infection in pregnancy is associated with high rates of gestational complications and preterm labor. Gastroenterology, (2006); 130(4): 1129-1134.
- Ornoy A, Tenenbaum A. Pregnancy outcome following infections by coxsackie, echo, measles, mumps, hepatitis, polio and encephalitis viruses. Reproductive Toxicology, (2006); 21(4): 446-457.
- Tse KY, Ho LF, Lao T. The impact of maternal HBsAg carrier status on pregnancy outcomes: a case–control study. Journal of hepatology, (2005); 43(5): 771-775.
- Elsheikh RM, Daak AA, Elsheikh MA, Karsany MS, Adam, I. Hepatitis B virus and hepatitis C virus in pregnant Sudanese women. Virology Journal, (2007); 4(1): 1.
- Hadzic N. Hepatitis C in pregnancy. Archives of Disease in Childhood-Fetal and Neonatal Edition, (2001); 84(3): F201-F204.
- Resti M, Azzari C, Mannelli F, Moriondo M, Novembre E, et al. Mother to child transmission of hepatitis C virus: prospective study of risk factors and timing of infection in children born to women seronegative for HIV-1. BMJ, (1998); 317(7156): 437-441.
- Shah NH, Shabbeir G. A review of published literature on hepatitis B and C virus prevalence in Pakistan. (2002).
- Garner JJ, Gaughwin M, Dodding J, Wilson K. Prevalence of hepatitis C infection in pregnant women in South Australia. The Medical journal of Australia, (1997); 167(9): 470-472.
- Irfan A, Arfeen S. Hepatitis C virus infection in spouses. Pakistan Journal of Medical Research, (2004); 43(3): 113-6.
- Khokhar N, Gill ML, Malik GJ. General seroprevalence of hepatitis C and hepatitis B virus infections in population. Journal of the College of Physicians and Surgeons–Pakistan, (2004); 14(9): 534-536.
- Almani SA, Memon AS, Qureshi AF, Memon NM. Hepatitis viral status in Sindh. Professional Medical Journal, (2002); 9(1): 36-43.
- Mast EE. Mother-to-infant hepatitis C virus transmission and breastfeeding. In Protecting Infants through Human Milk. In: Protecting Infants through Human Milk Springer US, (2004); 211-216.
- Muhammad N, Jan MA. Frequency of hepatitis "C" in Buner, NWFP. Journal of the College of Physicians and Surgeons Pakistan, (2005); 15(1): 11-14.
- Batash S, Khaykis I, Raicht RF, Bini EJ. High prevalence of hepatitis C virus infection among immigrants from the former Soviet Union in the New York City metropolitan area: results of a community-based screening program. The American journal of Gastroenterology, (2008); 103(4): 922-927.
- Cacoub P, Ohayon V, Sekkat S, Dumont B, Sbai A, et al. Epidemiologic and virologic study of hepatitis C virus infections in Morocco. Gastroenterologie clinique et biologique, (2000); 24(2): 169-173.
- Nafeh MA, Medhat A, Shehata M, Mikhail NN, Swifee Y, et al. Hepatitis C in a community in Upper Egypt: I. Cross-sectional survey. The American journal of tropical medicine and hygiene, (2000); 63(5): 236-241.
- Delage G, Infante–Rivard C, Chiavetta JA, Willems B, Pi D, et al. Risk factors for acquisition of hepatitis C virus infection in blood donors: results of a case-control study. Gastroenterology, (1999); 116(4): 893-899.
- Hutchinson SJ, Goldberg DJ, King M, Cameron SO, Shaw LE, et al. Hepatitis C virus among childbearing women in Scotland: prevalence, deprivation, and diagnosis. Gut, (2004); 53(4): 593-598.
![]()
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0


