

Full Length Research Article
Frequencies and clinical characteristics of common fusion oncogenes in core-binding factor Acute Myeloid Leukemia from Lahore Pakistan
Zafar Iqbal1*, Muhammad Absar2, Masood Shammas3, Nawaf Alanazi4, Salman Basit5, Khalid Aljarrah6, Sana Bilal7, Mona Elsafadi8, Abdulaziz Siyal8, Amer Mahmood8
Adv. life sci., vol. 8, no. 4, pp. 387-395, December 2021
*– Corresponding Author: Zafar Iqbal (Email: iqbalz@ksau-hs.edu.sa)
Authors' Affiliations
2. Hematology Oncology and Pharmacogenetics Engineering Sciences (HOPES) Group, Health Sciences Research Laboratories, Department of Zoology, University of the Punjab, Lahore – Pakistan
3. Department of Medical Oncology, Dana-Farber (Harvard) Cancer Institute, University of Harvard, Boston – USA
4. Cancer and Medical Genetics, CAMS-A, King Saud Bin Abdulaziz University for Health Sciences & King Abdullah International Medical Research Centre (KAIMRC), King Abdulaziz Medical City, National Guard Health Affairs, Al Ahsa -Saudi Arabia
5. Center for Genetics and Inherited Diseases, Taibah University, Almadinah Almunawwarah – Saudi Arabia
6. KSAUHS & Jordan University of Science and Technology – Saudi Arabia
7. Dept of Zoology, University of the Punjab Lahore – Pakistan
8. Stem Cell Unit Department of Anatomy, College of Medicine King Saud University – Saudi Arabia
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Acute myeloid leukemia (AML) is one of the most common blood cancers among adults. Genetic abnormalities associated with core-binding factor AML (CBF-AML) help in accurate diagnosis and prognostic stratification, and therefore help in clinical management of the disease. No studies have been carried out about frequencies of genetic abnormalities of CBF-AML and their association with clinical parameters in Lahore region of Pakistan. Therefore, objective of this study was to carry out genetic and characterization of CBF-AML.
Methods: The blood samples were collected along with clinical data AML patients from different hospitals of Lahore Pakistan July 2010 to Dec. 2020. RNA was extracted and RT-PCR was employed to detect CBF-AML -associated fusion oncogenes (AML1-ETO and CBFB-MYH11). Data was analyzed using SPSS version 25.
Results: Frequencies of AML1-ETO and CBFB-MYH11 were 13.6% and 11.4%, respectively. AML1-ETO had significant association with FAB subtype AML-M2, occupational exposure to chemical solvents and exposure to petrol products. One the other hand, CBFB-MYH11 was significantly associated with splenomegaly, FAB subtype AML-M4 patients and insecticides exposure.
Conclusions: Our results show that overall frequencies AML1-ETO and CBFB-MYH11 and hence CBF-AML is comparable to other ethnic groups. Correlation of specific genetic abnormalities with exposures to chemicals indicates a strong interplay between AML genetics and pollutants. This study will help not only in differential diagnosis and prognostic stratification of AML in Pakistan, but it also opens new windows to better understand biology of AML in correlation with environmental exposure.
Keywords: Acute Myeloid Leukemia; Genetic abnormalities; Core-binding factor leukemia, Prognostic stratification; environmental exposure
Introduction![]()
Among all hematopoietic diseases, the acute myeloid leukemia is most common clinical and biological disorder [1,2]. The incidence of (AML) acute myeloid leukemia is 3-4/100,000 people per year [3]. In acute myeloid leukemia (AML), abnormal blood cell (blast cells) production is caused by the crowding of nonfunctional cells in the blood and bone marrow [4]. The main symptoms of acute myeloid leukemia are fatigue, shortness of breath, anemia, gum bleeding, petechiae, which are caused by low production of functional white blood cells (WBC) and red blood cells (RBCs) with more chances of other infections [5]. The AML patient’s median age is approximately 70 years globally, so the prevalence of acute myeloid leukemia (AML) increases with age [6]. The exact cause of leukemia is still not clear, so, it spread and progresses in body very quickly if it left untreated [5].
The World Health Organization (WHO) classifies AML into several categories based on underlying genetic alterations to facilitate diagnosis and prognosis [7]. Recurrent genetic alterations are frequently observed in AML patients. Among them t (8;21) (q22; q22) and inv (16) (p13q22)/t (16;16) (p13q22) are the most common and result in generation of corresponding abnormal fusion genes RUNX1–RUNX1T1 and CBFB–MYH11 [8], respectively.
Acute myeloid leukemia (AML) with t (8;21) or inv (16) have been recognized as unique entities within AML and are usually reported together as core binding factor AML (CBF-AML). Core binding factor (CBF) is a heterodimeric protein complex involved in the transcriptional regulation of normal hematopoiesis. Mutations in CBF-encoding genes result in leukemogenic proliferative advantages and impaired differentiation of the hematopoietic progenitors. CBF molecular aberrations are responsible for approximately 20% of all adult acute myeloid leukemia (AML). Although CBF-AMLs are considered to have relatively good prognosis compared to other leukemia subtypes, they are a heterogeneous group of disorders and modern therapy frequently leads to relapse and the associated morbidity and mortality [9]. As no further studies have been carried out regarding molecular biology and clinical characteristics of CBF-AML, the objective of this study was to find out frequencies of fusion oncogenes in CBF-ABL and their correlation with demographic data, clinical parameters, and environmental exposure.
Methods![]()
Peripheral blood samples were obtained from of 132 acute myeloid leukemia (AML) patients admitted to the different hospitals of Lahore, Pakistan. A data form was filled about the queries of patients regarding demographic and clinical features before sampling. The blood sample (3ml) was drawn from acute myeloid leukemia (AML) patients and then poured in to the EDTA tubes and stored at -40̊C to maintain its integrity normal. For the detection of most common fusion oncogenes, i.e., AML1-ETO and CBFB-MYH11, the RT-PCR protocol was optimized. Informed consent from patients was taken for this study.
RNA Extraction
For total RNA extraction from blood sample, the TRIzol reagent method was opted from Chomczynski and Sacchi [10] and verified with little optimizing modifications by Iqbal et al. [11]. The main steps of RNA extraction consisted of lysis, isolation, precipitation, washing and solubilization. 750μl of TRIzol-LS reagent (MRC/USA) was mixed in to the 250μl of blood sample and kept it at room temperature for 5 minutes, then added 200μl of chloroform and vortex for 10 seconds, then left it for 15 minutes at room temperature, and centrifuged it in centrifugation machine (Sigma, 2-16 PK) at 4̊C, 14,000 rounds per minute (rpm) for 15 minutes. The RNA, present in the upper most clear aqueous phase was separated and then transferred to another clean Eppendorf. RNA was precipitated by adding 500μl of chilled isopropanol and mixed well for 5-10 minutes. After keeping it at room temperature for 5 minutes, Centrifuged it for 10 minutes at 14,000 rpm. A gel-like white pellet that was RNA precipitate, formed at the base of the Eppendorf. RNA pellet was resuspended in 1ml of 75% of ethanol after the removal of supernatant and vortex it and then again centrifuged it at 14,000 rpm for 10 minutes at 4-5̊C. After the removal of ethanol, the RNA pellets were air-dried for 15 minutes and keep Eppendorf inverted for 3-5 minutes. Then dissolved the RNA in 50 µl of diethyl pyrocarbonate (DEPC) treated water through a pipette tip. Incubated at 55-60̊C for 10-15 minutes and stored at -20̊C. To check the integrity of ribonucleic acid (RNA), extracted RNA was run on 1% agarose gel, and found the bands for 18S and 28s ribosomal RNA (rRNA). These prominent bands showed the best quality for the RT-PCR reaction.
Complementary Deoxyribonucleic acid (cDNA) Synthesis
The RNA was reverse transcribed to cDNA through the reverse transcribed (RT) reaction, which was catalyzed by enzyme “Reverse transcriptase” in the presence of random hexamer primers. The template was then used in PCR reaction. RT reaction protocol and other reaction conditions were adopted from Van Dongen [12]. Briefly 10μl of RNA was added to 10μl of RT-reaction mixture containing 5X RT Buffer, 25 mM dNTP Mix, 10mM Random hexamer primer, RiboLockTM RNase Inhibitor, M-MLV Reverse Transcriptase, DEPC-treated / nuclease free water. The reaction was carried out by incubating mixture of template, random hexamers and DEPC treated water at 70°C for 10 min. Then added rest of reagents and incubated at 42°C for 60 minutes, 70°C for 10 minutes and hold at 40°C in the last step [13]. The quality of cDNA was checked by amplification of housekeeping genes glyceraldehyde 3-phosphate dehydrogenase (GAPDH). Gene expression analysis at conventional PCR was performed by using 2µl cDNA on optimized conditions, using the synthesized gene specific primers [14].
Reverse Transcriptase PCR Amplifications
The PCR primers and nested PCR protocol used for the detection of AML1-ETO and CBFB-MYH11 fusion oncogenes were adopted from Van Dongen et al., [12]. In the 1st round of nested PCR, a 50 µl PCR reaction was performed containing 5x PCR buffer with KCl, 25Mm MgCl2, 10mM dNTP Mix, DEPC Water, Taq DNA Polymerase (forward primer and reverse primer) and template of cDNA. The same test was performed in round 2nd with the cDNA template being the product of round 1st. Thermal cycling steps for nested PCR were preliminary denaturation at 95°C for 30 sec followed by 35 cycles of denaturation of double stranded DNA at 95°C for 30 sec, annealing of primers to DNA template at 65°C for 60 sec and extension to form multiple copies of DNA strands at 72°C for 60 sec, followed by a final extension at 72°C for 07 minutes. The 2nd round PCR was carried out with the same conditions. The final PCR products was run on 2% agarose gel, after staining with 3% ethidium bromide, then visualized under ultraviolet (UV) light [15].
Data Analysis
In this study, SPSS version 25 was used for data analysis. To determine the association between fusion oncogenes and different variables “chi square test” was used [16], and where the expected count was less than 5, the “Fishers Exact test” was used. Significant p-value was considered which was below than or equal to 0.05.
Results
![]()
According to the final analysis, a total of 132 acute myeloid leukemia (AML) patients were included, in which, 77 (58.33%) were males, and 55 (41.67%) were the females. Out of 77 (58.33%) males, 9 (6.8%) were in age group of 1-16 years, 48(36.4%) were in 17-59 year, and 20 (15.1%) were in ≥60 years age group. Whereas, out of 55 (41.67%) females, 5 (15.6%) were in age group of 1-16 years, 34(25.8%) were in 17-59 year, and 16 (12.1%) were in ≥60 years age group. it was also found that among age groups, the 17-59 years age group was quite different, because its number of patients/ percentages was highest as 82/132 (62.2%), as compared to other age group, that was 14(10.61%) in age group of 1-16 years, and 36 (27.27%) was in group of ≥60.
According to the recorded clinical and demographic, it was observed that the anemia/paleness, shortness of breath, fatigue and fever were the main symptoms in a total of 132 (AML) patients, which were 83.9%, 69.8%, 63.1%, 59.7% respectively. 67.8% of the patients have symptoms of weight loss/ loss of appetite at time of presentation. While the chloroma (6.7%) and lymph node swelling (15.2%), were amongst the lowest recorded symptoms. Easy Bruising or Bleeding (60.4%), bone and joint pain (65.1%), and blast cells (66%) were recorded. 28 (21.21%) were hepatomegaly positive AML patients, which was highest as compared to the splenomegaly and lymphadenopathy. Whereas 16 (12.21%) were recorded as splenomegaly positive whereas, 20 (15.2%) were lymphadenopathy. Total leucocytes count (TLC) of 73 (55.3%) out of 132 AML patients, was <30,000 and 59 (44.7%) were >30,000. In 41/132 (31.10%) of AML patients, platelets count was <30,000 and 91 (68.9%) were >30,000. Present data revealed that acute myeloid leukemia (AML) patients having occupational exposure to mutagenic exposures like, chemical solvent, that was 18.9%, insecticide (7.6%), petrol products (11.4%), while the percentage of AML patients having no exposure, (62%) were recorded as highest. The types of patients were recorded as per French-American-British (FAB) classification. The two types of AML–M2 (33.6%) and AML-M4 (29.5 %) were observed as highest, respectively. Whereas AML-M0 (8.3%), AML-M1 (9.1%), AML-M3 (10.6%), AML-M5 (6.8%), AML-M6 (1.5%), AML-M7 (0.8%) were recorded.
Molecular Analysis
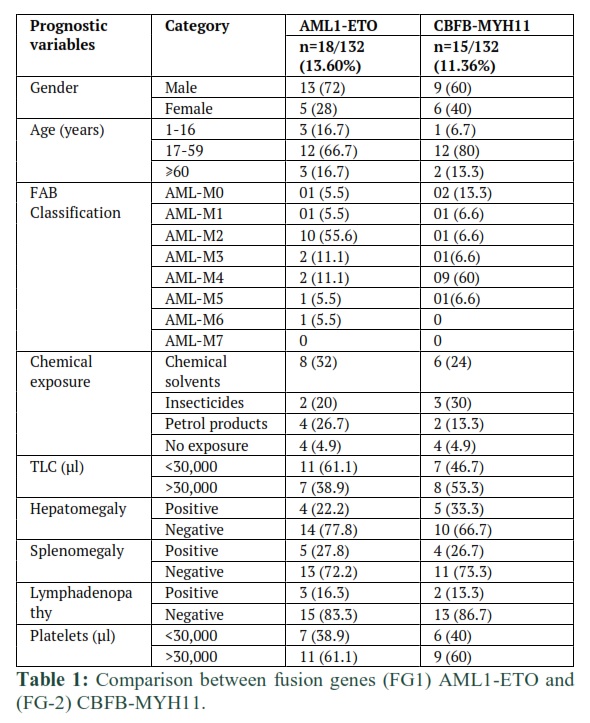
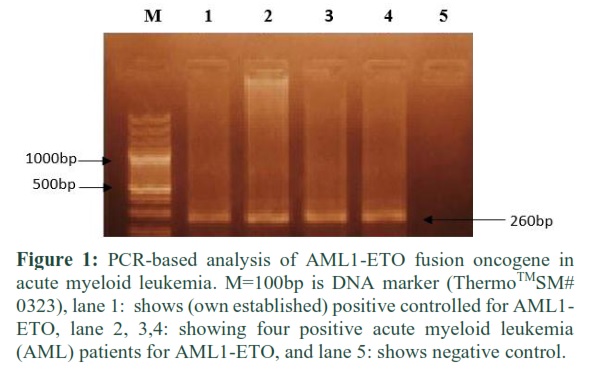
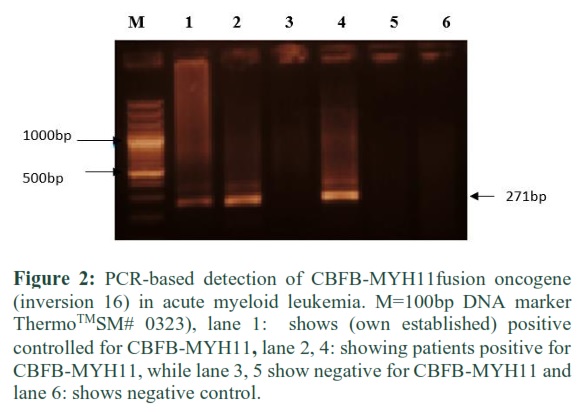
A total of 132 AML samples were processed for molecular analysis. AML1-ETO fusion oncogene (FG-1) was detected in 18/132 (13.6%) AML patients while CBFB-MYH11 fusion transcript (FG-2) was detected in 15/132 (11.4%) blood samples of (AML) patients (Figures 1 & 2).
Statistical Analysis and comparison between Fusion Genes (FG-1) and (FG-2)
According to this research, the fusion gene (FG-1) AML1-ETO was compared with (FG-2) CBFB-MYH11 in patients with acute myeloid leukemia (AML) in relation to its all mentioned prognostic variable. It was found that the FAB classification is a significant prognostic variable. The significant p-values in FAB type of AML- M2 (0.003*) for fusion gene (FG-1) and AML-M4 (0.008*) for fusion gene (FG-2) were observed (Table 1).
Statistical Analysis of Fusion Genes (FG-1) and (FG-2) with CBF-AML –VE Patients
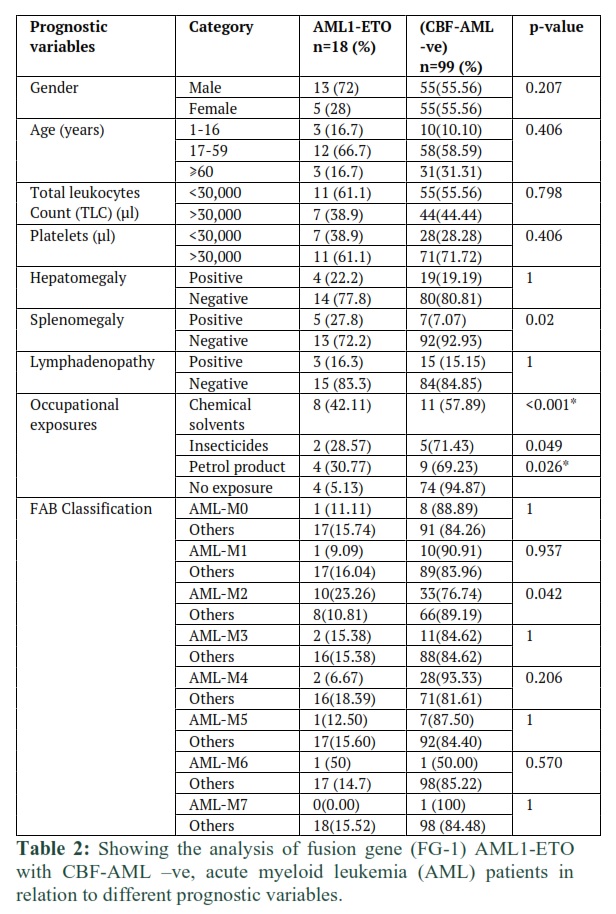
The fusion gene (FG-1) AML1-ETO was compared with CBF-negative group of patients with acute myeloid leukemia (AML) in relation to different prognostic variables. It was observed that fusion oncogene (FG-1) AML1-ETO was positive in 8/18(42.11%) acute myeloid leukemia (AML) patients exposed to chemical solvent the association between exposure to chemical solvent and which was statistically significant (p-value <0.001*). Similarly (FG-1) AML1-ETO was positive in 4(30.77%) (AML) patients exposed to petrol products, the association between petrol products and AML1-ETO (FG-1) was also statistically significant (p-value 0.026*). Whereas AML1-ETO (FG-1) was positive in only 2(28.57%) (AML) patients exposed to insecticides, which was not statistically significant (Table 2).
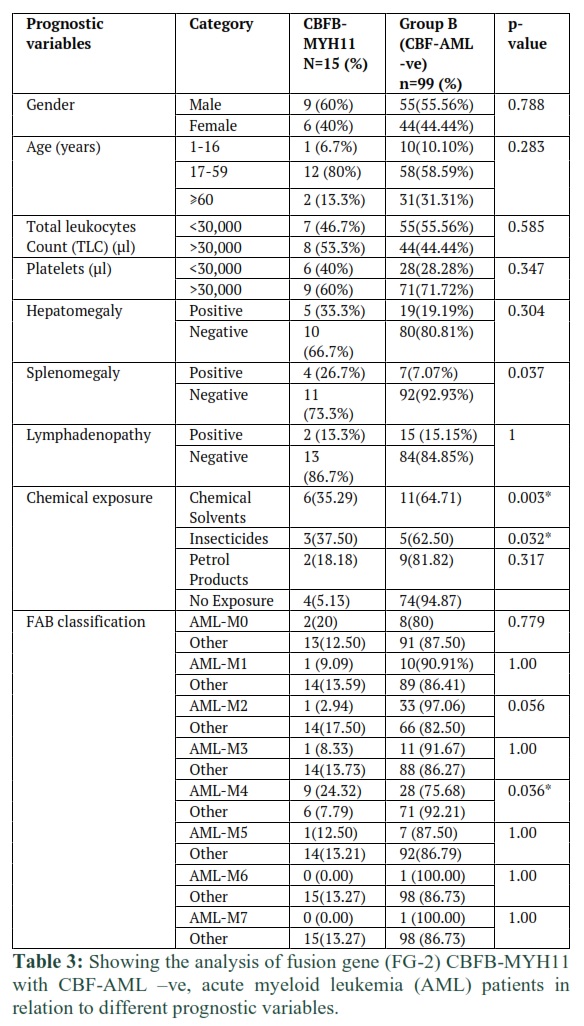
The fusion gene (FG-2) CBFB-MHY11 was also compared with CBF-negative group of patients with acute myeloid leukemia (AML) in relation to different prognostic variables. It was observed that the fusion oncogene CBFB-MHY11 (FG-2) was positive in 6(35.29%) (AML) patients exposed to chemical solvent. Similarly, 3(37.50%) patients were exposed to insecticides and 2(18.18%) were exposed to petrol products. Chemical solvent (p-value 0.003*) and insecticides (p-value 0.032*) were statistically significantly associated with CBFB-MHY11 (FG-2) (Table 3). It was also observed that FAB classification type AML-M4 was statistically significant prognostic variable, with p-value (0.036*) (Table 3).
Statistical Analysis of Group A (CBF-AML) and Group B (CBF-AML negative) Acute Myeloid Leukemia Patients
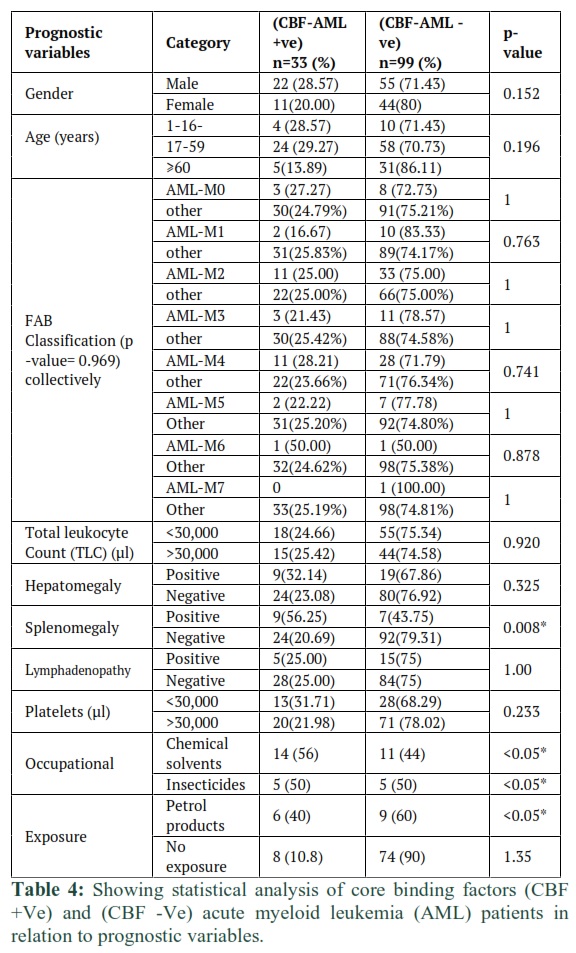
The Group A (CBF-AML) was also compared with Group B (CBF-AML-negative) in relation to different prognostic variables. It was observed that Splenomegaly was statistically significantly associated with the fusion oncogenes (p-value 0.008*). The measured relative risk of Splenomegaly was 4.93(1.66-14.59) higher in CBF-AML as compared to CBF-AML-negative (Table 4). The p-value for occupational exposures was also recorded as <0.05* when CBF-AML patients were compared with CBF-negative AML patients (Table 4).
AML1-ETO (FG-1): Among 132 acute myeloid leukemia (AML) patients, fusion oncogene (FG-1) AML1-ETO was 18 (13.64%), harbor this translocation, i.e., t (8;21) (q22; q22). Its distribution was 3/18 (16.67%) in the age group 1-16 years, 12/18 (66.67%) patients in the age group 17-59 years and 3/18 (16.67%) patients of ≥60 years age group. In patients, male to female ratio was detected 2.6:1. Thus, 13/18 (72.2%) males and 5/18 (27.7%) females were found. 8(61.5%) of males and 4 (80%) of females in age group of 17-59 years were recorded as highest in numbers, and 3 (23.1%) males in age group 1-16 years, and 2 (15.4%) of males and 1 (20%) of females in age group ≥60 years were observed. The association of fusion genes regarding age and gender is not statistically significant (p-value 0.485) and relative risk was measured (RR 1.3 (0.6235, 2.711).
Five (27.8%) AML patients were positive for splenomegaly, while 3 (16.3%) were recorded positive for lymphadenopathy and 4/18 (22.22%) patients were hepatomegaly positive. The total leucocytes count (<30,000µl) was observed in 11 (61.1%) patients, and 7 (38.9%) were in (>30,000µl) category. While the platelets count (<30,000µl) was recorded in 7 (38.9%) and 11 (61.1%) were in (>30,000µl) category. Out of 18 patients (FG-1) AML1-ETO 8 (32%) patients were associated with chemical solvent, 2 (20%) had exposure to insecticides, 4 (26.7%) having association with petrol products and 4 (4.9%) had no occupational exposure to potential mutagenic agent. Out of 18 patients with having fusion gene (FG-1) AML1-ETO, 10 (55.6 %) were recorded as highest in number as AML-M2, while AML-M0 and AML-M1, AML-M5, AML-M6 were 01 (5.5%), AML-M3 and AML-M4were 2 (11.1%) were, whereas AML-M7 was nil.
CBFB-MYH11 (FG-2): 15/132 (11.36%), acute myeloid leukemia (AML) patients carried Inv (16) (p13, q22) chromosomal translocation of fusion oncogene (FG-2) CBFB-MYH11. Its distribution was recorded, that is 1/15 (6.67%) Patients with age group of 1-16 years, 12/15 (80%) fall in the 17-59 years age group range and 2/15 (13.35%) was ≥60. Among 15 patients, 9 were males (60%) and 6 (40%) were females. 7 (77.8%) of males and 5 (83.3%) of females in age group of 17-59 years were recorded as highest in numbers, and 1 (11.1%) male in age group 1-16 years, and 1 (11.1%) of males and 1 (16.7%) of females in age group ≥ 60 years were observed. The association of fusion genes and age and gender is not statistically significant (p-value 0.485) and relative risk was measured (RR 1.3 (0.6235, 2.711). 5 (33.3%) were hepatomegaly positive, 4 (26.7%) were positive for splenomegaly, while 2 (13.3%) were recorded positive for lymphadenopathy. the total leucocytes count (<30,000µl) was recorded in 7 (46.7%) patients, and 8 (53.3%) were in (>30,000µl) category. Whereas the platelets count (<30,000µl) was recorded in 6 (40%) and 9 (60%) were in (>30,000µl) category. 6 (24%) patients were associated with chemical solvent, 3 (30%) had exposure to insecticides, 2 (13.3%) having association with petrol products and 4 (4.9%) had no occupational exposure to potential mutagenic agent. The patients with having fusion oncogenes (FG-2) CBFB-MYH11, 9/15 were recorded as highest as AML-M4, while 02/15 (13.3%) were AML-M0, and 01/15 (6.7%) were AML-M1, AML-M2, AML-M3, AML-M5, while no patient with AML-M6, and AML-M7 were recorded.
Overall, we conclude that frequency of CBF-AML (AML1-ETO and CBFB-MYH11) is in accordance with reports from other countries. Correlation of specific genetic abnormalities with exposures to chemicals hints at a strong interplay between different genetic lesions and exposure to pollutants, that may help in finding out factors initiating AML. This study will help not only in differential diagnosis and prognostic stratification of AML in Pakistan, but it also opens new windows to better understand biology of AML in correlation with environmental exposure.
Figures & Tables
Discussion![]()
Acute myeloid leukemia, (AML) is a heterogeneous disease, and this heterogeneity is caused by its genetic and geographical differences between various populations [17,18]. In this research, blood samples of acute myeloid leukemia (AML) patients were used for molecular analysis through RNA extraction in RT-PCR, because bone marrow samples are difficult to get. Europe-against-Cancer (EAC) protocol and others showed that the samples of blood and marrow produce same results [19,20]. In 2006, a meeting at NIH Bethesda USA also confirmed the blood samples as a best choice for the purpose of management and detection of the disease [21]. In this study the blood samples were collected in EDTA, because it was reported that, blood collection in EDTA is the best choice for RNA and it was also suggested that samples should be analyzed within 1 day after collection [21]. In this study, white blood cells were used for mRNA extraction, which was more feasible, because Hughes et al., reported the WBCs better as better than using mononuclear cells (MN). The report translates “The use of Ficoll is not recommended because use of fractionated leukocytes is less sensitive than analyses based on total leukocytes following red-cell lysis”. Many other researchers reported the use of whole WBCs [20,21]. Extreme care was taken in completing the tests on the samples to minimize mRNA degradation. Hughes et al., [21] recommended that samples should be processed within 24 hours of collection while Muller et al., [22] have also reported that RNA degradation in unstabilized peripheral blood samples does not play a major role in sample being processed on the day of blood collection for minimal residual disease studies in Leukemia. In present work, validated Reverse-transcriptase PCR (RT-PCR) protocol was used [15] and even at present workplace previously [23]. Furthermore, for detection of fusion genes, it is quite common protocol used in the USA, Europe and other developed countries [24-26]. To reduce the possibility of PCR product carryover and contamination, the best measure was taken include to select separate area for RNA isolation, preparation of PCR master mix, Poly erase chain reaction, and all other measures to control for contamination [27]. Our successful results show the authenticity of present work and accuracy of the protocol developed by Van Dongen et al., [12]. In leukemia patients, the most common fusion genes are produced in the result of various genetic / chromosomal abnormalities [28]. The 4 most common translocations are between 4% and 10% and these most common fusion oncoproteins are AML1-ETO, CBFB-MYH11, PML-RARα and MLL fusions [29]. Core-binding factor (CBF) of acute myeloid leukemia (AML) is cytogenetically defined by the presence of t (8;21) (q22; q22) AML1-ETO or inv (16) (p13q22)/t (16;16) (p13; q22) CBFB-MYH11, commonly abbreviated as t (8;21) and inv (16), respectively. In both subtypes, the cytogenetic rearrangements disrupt genes that encode subunits of core-binding factor, a transcription factor that functions as an essential regulator of normal hematopoiesis. The rearrangements t (8;21) and inv (16) involve the RUNX1/RUNX1T1 (AML1-ETO) and CBFB/MYH11 genes, respectively [30].
Present study reports the prevalence of the two most common fusion oncogenes, i.e., AML1-ETO and CBFβ-MYH11. It was found that 33/132 (25%) acute myeloid leukemia (AML) patients had one of these two fusion oncogenes with the incidence of CBFβ-MYH11 in 15/132 (11.4%) patients, and AML1-ETO in 18/132 (13.6%) patients. according to other published data, the t (8;21) translocation is detected in 8-12% of AML patients and 10%–22% of cases with FAB subtype M2 and the frequency decreases with age, accordingly, t (8;21) is most common in younger patients and rare in patients over 60 years [31]. It may be difficult to recognize acute myeloid leukemia (AML) through symptoms because there might be not any specific symptoms as AML initiates suddenly [32,33]. The main AML symptoms in present study were paleness /Anemia (63.1%) , shortness of breath (69.8%), fatigue (63%) and easy bruising/ bleeding (60.4%) were the main symptoms that were recorded in the acute myeloid leukemia (AML) patients and it is in consensus with the previous work in Pakistan, i.e. fever (72.8%), general weakness (60%), gum bleeding (37.6%) and dyspnea (12%) [34], while chloroma 10/132 (6.7%) were amongst the lowest recorded symptoms.
The overall incidence of AML increases with age; it is a disease of the elder age, with a median age (~70 years) [35]. Age at diagnosis is favorable prognostic factor [36]. According to our research, the 24/33 (72.7%) AML patients with having fusion genes AML-ETO1 and CBFB-MYH11, and (62.12%) were of total AML patients in the age group of (17-59 years), AML is more common in male than female with ratio of ~2:1 [37]. Similarly in this study male AML patients were (58.33%) and females were (41.67%). In case of fusion gene (FG-1) AML1-ET0, the males were (66.67%) highest than females (23.1). Whereas, in case of AML patients with fusion oncogenes (FG-2) CBFB-MYH11, the female patients (83.3%) were highest in number, and male were (77.8%) but not statistically significant. According to this research, the fusion gene (FG-1) AML1-ETO was compared with (FG-2) CBFB-MYH11 in patients with acute myeloid leukemia (AML). It was found that the FAB classification is a significant prognostic variable. The significant p-values in FAB type of AML-M2 (0.003*) for fusion gene (FG-1) and AML-M4 (0.008*) for fusion gene (FG-2) were observed. The results were also compared with other published data, which also showed similarities, i.e., The AML1–ETO fusion gene was detected up 50% of the M2 subgroup and absent in the M1 and M4 subtypes and healthy controls [38].
The fusion gene (FG-1) AML1-ETO was also compared with CBF-negative group of patients with acute myeloid leukemia (AML). The occupational exposure was observed as significant prognostic variable having p-value i.e., <0.001* and 0.026* of chemical solutions and petrol products, respectively. While when fusion gene (FG-2) CBFB-MYH11 was compared with CBF-negative group of patients with acute myeloid leukemia (AML), it was found that the chemical solvents and insecticide as a chemical exposure have significant prognostic impact. The p-values (0.003*) for chemical solvents and (0.056*) for insecticides were recorded. The patients who had more exposure to chemical solvents, insecticide, and petrol product have the significant chance of AML. These exposures were also significant to fusion genes, AML1-ETO and CBFB-MYH11. The p-value for occupational exposures was recorded <0.05* when CBF-AML patients were compared with CBF-negative AML patients. As it was also reported by other researchers that the exposures are associated with an increased risk of AML (all subtypes combined) and/or individual subtypes included benzene, diesel fuel, metals, insecticides, fertilizers, glues and adhesives, paints and other coatings, and inks and pigments [39]. In Acute myeloid leukemia extramedullary infiltration by leukemic cells may cause lymphadenopathy, splenomegaly or hepatomegaly and lymphadenopathy is not as common as seen in acute lymphoblastic leukemia while, hepatosplenomegaly however is more frequent but massive hepatosplenomegaly is uncommon [40]. In this research, the clinical data of CBF-AML patients was compared with CBF-negative AML patients, and it was observed that the splenomegaly was a significant prognostic variable having p-value of (0.008*). As reported by Naghmi and Khalid, (2013), hepatomegaly and splenomegaly were observed in 48% and 45% patients respectively, while majority had mild to moderate hepatosplenomegaly [41].
This research study shows the prevalence of two common fusion genes and their association with clinical and demographical features. It also indicates that the patients can be categorized into different prognostic groups that based on molecular cytogenetic evaluation and its association with clinical characteristic. As our findings have similarities with previously reported studies or literature. More comprehensive and large-scale studies using advance genetic techniques like whole genome sequencing etc., are required to further explore the genetic heterogeneity of acute myeloid leukemia (AML) and its correlation with disease biology. Which will further help in better prognostic stratification and improvement in treatment outcome.
In conclusion, this is first study from Pakistan, which investigated the frequency of two common fusion oncogenes in AML patients, and their association/ correlation with clinical / demographical features. This research will help in the prognostic stratification and risk adapted management of AML patients.
Author Contributions
All of the work carried out is author’s original research data.
Author declares that he has no conflict of interest.
References
- Zhou M-h, Gao L, Jing Y, Xu Y-y, Ding Y, et al. Detection of ETV6 gene rearrangements in adult acute lymphoblastic leukemia. Annals of hematology, (2012); 91(8): 1235-1243.
- Ahmad F, Mohota R, Sanap S, Mandava S, Das BR. Molecular evaluation of DNMT3A and IDH1/2 gene mutation: frequency, distribution pattern and associations with additional molecular markers in normal karyotype Indian acute myeloid leukemia patients. Asian Pacific journal of cancer prevention, (2014); 15(3): 1247-1253.
- Schlenk RF. Post-remission therapy for acute myeloid leukemia. Haematologica, (2014); 99(11): 1663.
- Boileau M, Laverdière I, Mitchell A, Ng SW, Wang JC, et al. Identification of existing bioactive molecules that target acute myeloid leukemia stem cells. Experimental Hematology, (2016); 44(9): S60-S61.
- Döhner H, Weisdorf DJ, Bloomfield CD. Acute myeloid leukemia. New England Journal of Medicine, (2015); 373(12): 1136-1152.
- Ossenkoppele G, Löwenberg B. How I treat the older patient with acute myeloid leukemia. Blood, The Journal of the American Society of Hematology, (2015); 125(5): 767-774.
- Falini B, Tiacci E, Martelli MP, Ascani S, Pileri SA. New classification of acute myeloid leukemia and precursor-related neoplasms: changes and unsolved issues. Discovery medicine, (2010); 10(53): 281-292.
- Speck NA, Gilliland DG. Core-binding factors in haematopoiesis and leukaemia. Nature Reviews Cancer, (2002); 2(7): 502-513.
- Sinha C, Cunningham LC, Liu PP. Core binding factor acute myeloid leukemia: new prognostic categories and therapeutic opportunities; 2015. Elsevier. pp. 215-222.
- Chomczynski P, Sacchi N. Single-step method of RNA isolation by acid guanidinium thiocyanate-phenol-chloroform extraction. Analytical biochemistry, (1987); 162(1): 156-159.
- Iqbal Z. Molecular Hematology in Leukemia Biology and Treatment: Past, Present, and Future. Journal of Applied Hematology, (2012); 3(2): 55.
- Van Dongen J, Macintyre E, Gabert J, Delabesse E, Rossi V, et al. Standardized RT-PCR analysis of fusion gene transcripts from chromosome aberrations in acute leukemia for detection of minimal residual disease. Leukemia, (1999); 13(12): 1901-1928.
- de Bont ES, Fidler V, Meeuwsen T, Scherpen F, Hählen K, et al. Vascular endothelial growth factor secretion is an independent prognostic factor for relapse-free survival in pediatric acute myeloid leukemia patients. Clinical Cancer Research, (2002); 8(9): 2856-2861.
- Barber RD, Harmer DW, Coleman RA, Clark BJ. GAPDH as a housekeeping gene: analysis of GAPDH mRNA expression in a panel of 72 human tissues. Physiological genomics, (2005); 21(3): 389-395.
- Lee PY, Costumbrado J, Hsu C-Y, Kim YH. Agarose gel electrophoresis for the separation of DNA fragments. JoVE (Journal of Visualized Experiments), (2012); (62): e3923.
- Zhang L, Cao Z, Ruan M, Zeng Q, Zhao L, et al. Monitoring the AML1/ETO fusion transcript to predict outcome in childhood acute myeloid leukemia. Pediatric blood & cancer, (2014); 61(10): 1761-1766.
- Treviño LR, Yang W, French D, Hunger SP, Carroll WL, et al. Germline genomic variants associated with childhood acute lymphoblastic leukemia. Nature genetics, (2009); 41(9): 1001-1005.
- Tong H, Lu C, Wang Q, Wang H, Wang H. Immunophenotype of Chinese patients with T-lineage acute lymphoblastic leukemia and its association to biological and clinical features. Acta haematologica, (2012); 127(4): 199-204.
- Kantarjian HM, Talpaz M, Cortes J, O’Brien S, Faderl S, et al. Quantitative polymerase chain reaction monitoring of BCR-ABL during therapy with imatinib mesylate (STI571; gleevec) in chronic-phase chronic myelogenous leukemia. Clinical cancer research, (2003); 9(1): 160-166.
- Branford S, Cross N, Hochhaus A, Radich J, Saglio G, et al. Rationale for the recommendations for harmonizing current methodology for detecting BCR-ABL transcripts in patients with chronic myeloid leukaemia. Leukemia, (2006); 20(11): 1925-1930.
- Hughes T, Deininger M, Hochhaus A, Branford S, Radich J, et al. Monitoring CML patients responding to treatment with tyrosine kinase inhibitors: review and recommendations for harmonizing current methodology for detecting BCR-ABL transcripts and kinase domain mutations and for expressing results. Blood, (2006); 108(1): 28-37.
- Müller M, Merx K, Weiβer A, Kreil S, Lahaye T, et al. Improvement of molecular monitoring of residual disease in leukemias by bedside RNA stabilization. Leukemia, (2002); 16(12): 2395-2399.
- Iqbal Z, Tanveer A. Incidence of different fusion oncogenes in acute Lymphoblastic Leukemia (ALL) patients from Pakistan: possible implications in differential diagnosis, prognosis, treatment and management of ALL. Haematologica, (2006); 9164.
- Agrawal S, Unterberg M, Koschmieder S, zur Stadt U, Brunnberg U, et al. DNA methylation of tumor suppressor genes in clinical remission predicts the relapse risk in acute myeloid leukemia. Cancer research, (2007); 67(3): 1370-1377.
- Fu J-F, Liang D-C, Shih L-Y. Analysis of acute leukemias with MLL/ENL fusion transcripts: identification of two novel breakpoints in ENL. American journal of clinical pathology, (2007); 127(1): 24-30.
- Imanishi H, Okamura N, Yagi M, Noro Y, Moriya Y, et al. Genetic polymorphisms associated with adverse events and elimination of methotrexate in childhood acute lymphoblastic leukemia and malignant lymphoma. Journal of human genetics, (2007); 52(2): 166-171.
- Kwok Sa, Higuchi R. Avoiding false positives with PCR. Nature, (1989); 339(6221): 237-238.
- Fielding AK. Current therapeutic strategies in adult acute lymphoblastic leukemia. Hematology/Oncology Clinics, (2011); 25(6): 1255-1279.
- Kumar CC. Genetic abnormalities and challenges in the treatment of acute myeloid leukemia. Genes & cancer, (2011); 2(2): 95-107.
- Sangle NA, Perkins SL. Core-binding factor acute myeloid leukemia. Archives of pathology & laboratory medicine, (2011); 135(11): 1504-1509.
- Reikvam H, Hatfield KJ, Kittang AO, Hovland R, Bruserud Ø. Acute myeloid leukemia with the t (8; 21) translocation: clinical consequences and biological implications. Journal of Biomedicine and Biotechnology, (2011); 2011.
- Han Y, Xue Y, Zhang J. Clinical and molecular cytogenetic studies of a case of B-lineage acute lymphoblastic leukemia with t (14; 14)(q11; q32). Zhonghua yi xue yi chuan xue za zhi= Zhonghua yixue yichuanxue zazhi= Chinese journal of medical genetics, (2012); 29(2): 137-140.
- Faiz M, Iqbal QJ, Qureshi A. High prevalence of BCR‐ABL fusion transcripts with poor prognostic impact among adult ALL patients: report from Pakistan. Asia‐Pacific Journal of Clinical Oncology, (2011); 7(1): 47-55.
- Sultan S, Zaheer HA, Irfan SM, Ashar S. Demographic and clinical characteristics of adult acute Myeloid Leukemia-tertiary care experience. Asian Pacific Journal of Cancer Prevention, (2016); 17(1): 357-360.
- Levis M, Ravandi F, Wang ES, Baer MR, Perl A, et al. Results from a randomized trial of salvage chemotherapy followed by lestaurtinib for patients with FLT3 mutant AML in first relapse. Blood, The Journal of the American Society of Hematology, (2011); 117(12): 3294-3301.
- Dores GM, Devesa SS, Curtis RE, Linet MS, Morton LM. Acute leukemia incidence and patient survival among children and adults in the United States, 2001-2007. Blood, The Journal of the American Society of Hematology, (2012); 119(1): 34-43.
- Harani MS, Adil S, Shaikh MU, Kakepoto GN, Khurshid M. Frequency of fab subtypes in acute myeloid leukemia patients at Aga Khan University Hospital Karachi. Journal of Ayub Medical College, (2005); 17(1): 26.
- Zidanloo SG, Colagar AH. Geographic heterogeneity of the AML1-ETO fusion gene in Iranian patients with acute myeloid leukemia. Reports of biochemistry & molecular biology, (2014); 3(1): 7.
- Wong O, Harris F, Armstrong TW, Hua F. A hospital-based case-control study of acute myeloid leukemia in Shanghai: analysis of environmental and occupational risk factors by subtypes of the WHO classification. Chemico-biological interactions, (2010); 184(1-2): 112-128.
- Kumar L, Menon H, Sharma A, Wadhwa J, Kumar R, et al. Acute myeloid leukemia (AML): A study of 516 patients. Journal of Clinical Oncology, (2004); 22(14_suppl): 6711-6711.
- Asif N, Hassan K. Acute myeloid leukemia amongst adults. Journal of Islamabad Medical and Dental College, (2013); 258-63.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0