

Full Length Research Article
Serum Anti-Nuclear Antibodies and their patterns on immunofluorescence in patients with joint pain from Lahore, Pakistan
Muhammad Daood Khan1, Bushra Mubarak1*, Kainat Waheed1, Iqra Munir1
Adv. life sci., vol. 9, no. 3, pp. 318-322, October 2022
*– Corresponding Author: Bushra Mubarak (Email: bushra.mubarik@yahoo.com)
Authors' Affiliations
[Date Received: 14/06/2022; Date Revised: 28/07/2022; Date Published: 31/10/2022]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Autoimmunity is the deviation of the immune system from its natural course and evoking a potent inflammatory response against organs or systems of its own body. Anti-nuclear antibodies (ANA) are an important marker for the diagnosis of autoimmune. The incidence of autoimmune diseases is increasing globally due to advancements in civilization, so it becomes crucial to monitor its trends. The current study aimed to determine the prevalence of ANA and its specific pattern in individuals with joint pain.
Methods: The duration of this cross-sectional study was 6 months, from December 2018 to May 2019. ANA profiles of 155 subjects were evaluated using the indirect immunofluorescence (IIF) technique.
Results: Amongst 155 enrolled subjects 101(65.2%) were females and 54(34.8%) were males. Rheumatoid factor was positive in 61 (39.3%) patients. ANA was found positive in 35 (22.5%) individuals, 5(14.3%) males, and 30(85.7%) females. Homogenous pattern was positive in 25(71.4%), 5(14.3%) fine speckled, 5(14.3%) centromere, and 1(2.8%) presented nuclear dots. The most frequent titer observed was 1/320 in 14(40%) individuals.
Conclusion: The homogenous pattern was frequently observed patterns ANA positive subjects. There was also a significant relationship between age group and their patterns. The homogenous pattern was most frequent among the 60-69-year age group.
Keywords: Autoimmunity; Immunofluorescence; Anti-nuclear antibody; Rheumatoid factor; Homogenous pattern; Inflammation
Introduction![]()
The immune system of our body works in a very precise way to eliminate pathogens and tumors that try to overwhelm a functioning body with their detrimental effects. However, the immune system is neither impeccable nor infallible, and sometimes it recognizes self-antigens and evokes a potent response against these self-antigens by self-reacting lymphocytes under the influence of some genetic and environmental factors, which is called autoimmunity. The central tolerance mechanism keeps in check reactive lymphocytes, but sometimes reactive lymphocytes manage to evade circulation[1]. The autoimmune regulator (AIRE) gene controls the negative selection. Thus defects in the AIRE gene can lead to the escape of reactive lymphocytes into circulation [2].
The autoimmune reaction can be organ specific like pernicious anemia, multiple sclerosis (MS), and Diabetes type 1, or systemic like systemic lupus erythematosus (SLE), Sjögren’s syndrome, and rheumatoid arthritis (RA) [1]. Alot of genetic polymorphisms in the gene regulators that control an immunological product are identified that play a role in the development of autoimmunity. Defects in cytokines and cytokine receptor genes can also cause autoimmunity [3]. In light of the evidence, autoimmune disorders can also be associated with one or more infections [4]. However, not all infections lead to autoimmunity as postulated by the hygiene hypothesis likewise normal flora in the gut also helps to evade autoimmune disorders [5]. Along with infections, and microbiota, dietary preferences of a population correlate with autoimmune diseases [6,7].
Anti-nuclear antibodies (ANA) are a heterogeneous group of antibodies that are directed against the nuclear material of a cell. These antibodies are clinically important, as they are present in most autoimmune diseases and their patterns assist in the diagnosis of different autoimmune diseases [8]. Presence of ANA is also observed in patients with hematological malignancies, chronic bacterial or viral infection, and in healthy individuals [9]. ANA are produced by autoreactive B cells as the consequence of the failure of self-tolerance [10]. ANA is performed on indirect immunofluorescence and the interpretation relies on the titer of antibodies in the patient's serum and the pattern of fluorescence using a fluorescent microscope.
A study in the United States reported a 13.8% prevalence of ANA with nuclear patterns (84.6%) was most frequently observed by Satoh M et al, followed by a cytoplasmic pattern (21.8%), and nucleolar patterns were least encountered [11]. In another study 3,127 individuals were enrolled and evaluated for their ANA profiles, out of a total 3,127, 494 were positive (15.8%). The most common pattern encountered was coarse speckled (31.2%), followed by nucleolar (18.0%), fine speckled (11.5%), and the least pattern observed was speckled [12]. With this background, the objective of the present study was to determine the prevalence of ANA and their specific pattern in individuals with joint pain.
Methods![]()
A descriptive study was conducted at the department of the University Institute of Medical Technology (UIMLT) on 155 patients with joint pain from December 2020 to May 2021. The study was approved by the Ethical review committee of the department. Written informed consent was signed by each patient before the collection of the sample. Male and female patients between 18 to 60 years presenting with joint pain and stiffness of phalangeal joints were included in the present study. Pregnant women and patients with confirmed autoimmune diseases were excluded.
Three (3) milliliter blood sample was collected from each subject by venipuncture technique. A slide agglutination test was used for Rheumatoid factor (RF) antibodies. For ANA evaluation qualitative and semi-quantitative indirect immune fluorescence test (Euroimmun mosaic basic profile) was used.
The principle involves the detection of autoantibodies, these autoantibodies attach to rat kidney and liver cells present on slides. After incubation, secondary antibodies (FITC) are added that will join to the primary antibody if the reaction is positive and the results are visualized by a fluorescent microscope. Reagents were prepared and the required volume of diluted sample (30µl per field 5×5 and 70µl per field 9×7) was placed on the reaction fields of the regent tray. A biochip was placed on the sample present on the reaction tray and the apparatus was incubated for 30 minutes at room temperature. After incubation, the slide was flushed with PBS-tween and then it was transferred to a cuvette containing PBS-tween. The slide was subjected to an appropriate amount of FICT (25µl per field 5×5 and 65µl per field 9×7) placed on the reagent tray after removing the biochip and incubated for 30 minutes at room temperature. Slides were washed again in new PBS-tween for 5 minutes. After washing the mounting media was applied to coverslips and placed on the biochip. The slides were then examined with a fluorescent microscope with a 40x objective lens setting.
Data were analyzed by IBM SPSS 25. Mean and ±SD are given for quantitative variables like age, and frequency and percentage are given for qualitative variables like genders. The Chi-square test was applied for the comparison of age groups with ANA positive patterns.
Results![]()
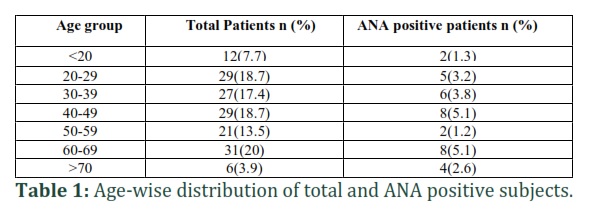
In the current study, a total of 155 individuals were enrolled. The mean age was 42.6 (± 16.3 SD). Amongst the total 155 subjects, 101(65.2%) were females and 54(34.8%) were males. The maximum number of individuals were from the 60-69 years age group 31(20%) followed by 20-29 years and 40-49 years age group, both encompassed 29(18.7%) individuals. In the >70-years group 6(3.9%) individuals were enrolled, and it was the least populated group.
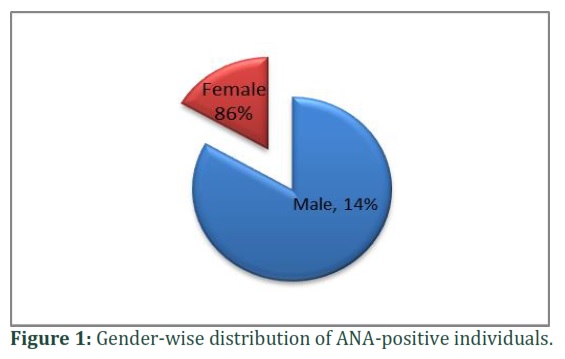
Results showed that 35(22.5%) subjects were positive for ANA. A total of 61 (39.3%) patients were positive for RF antibodies. Among total positive patients, 5 (14%) were males and 30(86%) were females (Fig 1).
The group 40-49 and 60-69 years had the maximum number of ANA-positive patients, both had 8(5.1%) subjects. The least frequency of ANA positivity recorded was amongst the <20-year age group which happened to be 2(13%) (Table 1).
The most frequent pattern observed in the present study was homogenous, which was observed in 25(71.4%) patients, followed by 5(14.3%) fine speckled. Coarse speckled was observed in 2(5.7%) patients, and a similar frequency of 2(5.7%) was observed for the centromere pattern. Only one patient showed a nuclear dots pattern, the least frequent pattern recorded (Fig 2).
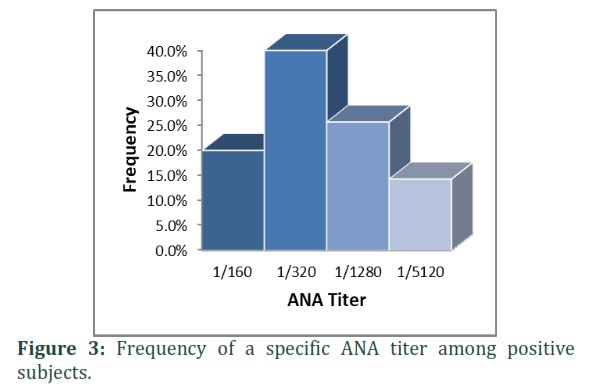
The most frequent titer observed in ANA-positive subjects was 1/320 observed in 14(40%) patients, followed by 1/1280, indicated by 9(25.7%) patients. Seven (20%) patients had a titer of 1/160, and the least frequent titer was 1/5120, observed in 5(14.3%) patients. There were no subjects (0%) with ANA titer of 1/80, 1/640, and 1/2560 among the studied individuals (Fig 3).
There was a significant relationship between age groups and ANA patterns (P-value 0.022). The age group 60-69 years presented a homogenous pattern in 7 individuals, and 6 individuals of 40-49 years were also positive. The fine speckled pattern was observed in younger groups, <20 years and 20-29 years age group, both had 2 positive cases. The nuclear pattern was only observed in a single individual from the 60-69 years age group.
The current study found a significant relationship between age and titer of ANA-positive patients (P-value 0.011). The age group 40-49 had the highest frequency, with 6 individuals recorded with 1/1280 titter. The group 30-39 years had 5 individuals presenting 1/320 titer, followed by 4 individuals from 60-69 years.
Figures & Tables

ANA test plays a vital role in the diagnosis of autoimmune diseases [13]. ANA was first described in 1948, and since then ANA are extensively used to diagnose autoimmune connective disorders such as SLE, Sjogren’s syndrome, and PM/DM [14]. The current study aimed to determine the prevalence of ANA and frequency of ANA patterns.
Sakthiswary and colleagues from Malaysia collected samples from 132 patients with primary osteoarthritis and documented that ANA was more prevalent among females 91 (68.9%) than males 41 (31.1%) [15]. Another study determined the prevalence of ANA in patients with joint pain from Taiwan and reported that among 515 total patients, 355 (65%) were positive for ANA test and females (80.8%) was more prevalent than male (19.2%) in ANA positive patients [16]. These results are in concordance with the current study indicating that out of 35 positive ANA individuals 30 (86%) were females and 5 (14%) were males.
In the present study, it was observed that the 40-49 and 60-69-year age groups encompassed a maximum number of ANA-positive patients. These results are in agreement with a study conducted by Mariz et al, in which the ANA positivity peaked in the 51-66-year age group reaching up to 20.8% in patients of autoimmune rheumatoid arthritis [17]. The most frequent pattern encountered in the present study was homogenous. The results of the current study are in accord with a study conducted by Swedish scientists on SLE patients, in which 54% of patients were presenting homogenous patents, 22% speckled, and 11% combined homogenous and speckled patterns, 9% nucleolar, and 1% presented centromere pattern [18]. A study from Germany reported the highest prevalence of granular patterns 71% was observed, followed by 19% homogenous, 2.6% nucleolar, and 0.7% centromere patterns out of 398 positive patients.16 Studies from Marin et al and Sharmin et al reported that the speckled pattern was predominant in 50.8% of individuals [19,20].
A study conducted to determine the prevalence of ANA in healthy Lebanese people found that the maximum number of subjects, 20% were positive for 1:100 titer. The minimum number of individuals, 1.1% had 1/1000 titer [21] as compared to the present study in which 1/320 was the frequent titer encountered in 40% of the ANA positive individuals.
Al-Mughales conducted a study to find the association of ANA patterns and their titers with the pathogenicity of SLE. They reported that speckled and homogenous patterns are more common in SLE patients [22] which is in agreement with the current study. A study on ANA patterns in patients with joint pain stated that most patients had uncommon nuclear, cytoplasmic, or mitotic sub-patterns. The least frequency of nuclear dots pattern was observed in these Indian patients [23].
Hayashi N and his coworkers did a study on ANA patterns in RA and healthy individuals in Japan. In healthy individuals, there was a 16.4% anti-dense fine speckled pattern (DFS) of antibodies was reported. In RA, 18.1% of DFS antibodies were observed [24] which is in concordance with the present study.
The correlation of ANA pattern and titer with systemic autoimmune rheumatic diseases (SARD) was shown by Wei et al. A titer of ≥1:320 described a PPV of 84.0% in SARD in the study. The mixed pattern was more frequent in SARD patients [25].
This study found that the prevalence of ANA was 22.5% among individuals suffering from joint pain. The ANA prevalence was mainly observed in the female group. The most frequent pattern was homogenous. There was also a significant relationship between age group and their ANA patterns. The homogenous pattern was the most frequent among the 60-69-year age group and fine speckled was the only observed pattern in the <20 groups.
Author Contributions
Muhammad Daood Khan: design, monitoring of subjects, participation in data acquisition, interpretation of results, drafting of manuscript.
Bushra Mubarak: conception, supervision of the project, analysis and interpretation of the results, writing and validation of the final version of the manuscript.
Kainat Waheed: analysis of results, statistical analysis, drafting of the manscript
Iqra Munir: statistical analysis, interpretation of results, validation of the final version of the manuscript.
![]()
All listed authors declare no conflict of interests in any capacity including competing and financial.
![]()
References
- Theofilopoulos AN, Kono DH, Baccala R. The multiple pathways to autoimmunity. Nature immunology, (2017); 18(7): 716-724.
- Klein L, Kyewski B, Allen PM, Hogquist KA. Positive and negative selection of the T cell repertoire: what thymocytes see (and don't see). Nature Reviews Immunology, (2014); 14(6): 377-391.
- Rosenblum MD, Remedios KA, Abbas AK. Mechanisms of human autoimmunity. The Journal of clinical investigation, (2015); 125(6): 2228-2233.
- Vojdani A. A potential link between environmental triggers and autoimmunity. Autoimmune diseases, (2014); 20(14): 283-291.
- Bach J-F. The hygiene hypothesis in autoimmunity: the role of pathogens and commensals. Nature Reviews Immunology, (2018); 18(2): 105-120.
- Jörg S, Grohme DA, Erzler M, Binsfeld M, Haghikia A, et al. Environmental factors in autoimmune diseases and their role in multiple sclerosis. Cellular and Molecular Life Sciences, (2016); 73(24): 4611-4622.
- Manzel A, Muller DN, Hafler DA, Erdman SE, Linker RA, et al. Role of “Western diet” in inflammatory autoimmune diseases. Current allergy and asthma reports, (2014); 14(1): 1-8.
- Pisetsky DS. Antinuclear antibody testing—misunderstood or misbegotten? Nature Reviews Rheumatology, (2017); 13(8): 495-502.
- Grygiel-Górniak B, Rogacka N, Puszczewicz M. Antinuclear antibodies in healthy people and non-rheumatic diseases–diagnostic and clinical implications. Reumatologia/Rheumatology, (2018); 56(4): 243-248.
- Faderl M, Klein F, Wirz OF, Heiler S, Albertí-Servera L, et al. Two distinct pathways in mice generate antinuclear antigen-reactive B cell repertoires. Frontiers in immunology, (2018); 9(16): 137-151.
- Satoh M, Chan EK, Ho LA, Rose KM, Parks CG, et al. Prevalence and sociodemographic correlates of antinuclear antibodies in the United States. Arthritis & Rheumatism, (2012); 64(7): 2319-2327.
- Mengeloglu Z, Tas T, Kocoglu E, Aktas G, Karabörk S. Determination of anti-nuclear antibody pattern distribution and clinical relationship. Pakistan journal of medical sciences, (2014); 30(2): 380-386.
- Konstantinov KN, Rubin RL. The universe of ANA testing: a case for point-of-care ANA testing. Autoimmunity Highlights, (2017); 8(1): 1-4.
- Kumar Y, Bhatia A, Minz RW. Antinuclear antibodies and their detection methods in diagnosis of connective tissue diseases: a journey revisited. Diagnostic pathology, (2009); 4(1): 1-10.
- Sakthiswary R, Rajalingam S, Norazman MR, Hussein H. Antinuclear antibodies in primary osteoarthritis of the knee: a case-control study. EXCLI journal, (2012); 7(6): 11624-11631.
- Wang K-Y, Yang Y-H, Chuang Y-H, Chan P-J, Yu H-H, et al. The initial manifestations and final diagnosis of patients with high and low titers of antinuclear antibodies after 6 months of follow-up. Journal of Microbiology, Immunology and Infection, (2011); 44(3): 222-228.
- Mariz HA, Sato EI, Barbosa SH, Rodrigues SH, Dellavance A, et al. Pattern on the antinuclear antibody–HEp‐2 test is a critical parameter for discriminating antinuclear antibody–positive healthy individuals and patients with autoimmune rheumatic diseases. Arthritis & Rheumatism, (2011); 63(1): 191-200.
- Frodlund M, Dahlström Ö, Kastbom A, Skogh T, Sjöwall C. Associations between antinuclear antibody staining patterns and clinical features of systemic lupus erythematosus: analysis of a regional Swedish register. BMJ open, (2013); 3(10): e003608.
- Marin GG, Cardiel MH, Cornejo H, Viveros ME. Prevalence of antinuclear antibodies in 3 groups of healthy individuals: blood donors, hospital personnel, and relatives of patients with autoimmune diseases. JCR: Journal of Clinical Rheumatology, (2009); 15(7): 325-329.
- Sharmin S, Ahmed S, Saleh AA, Rahman F, Choudhury M, et al. Association of immunofluorescence pattern of antinuclear antibody with specific autoantibodies in the Bangladeshi population. Bangladesh Medical Research Council Bulletin, (2014); 40(2): 74-78.
- Racoubian E, Zubaid RM, Shareef MA, Almawi WY. Prevalence of antinuclear antibodies in healthy Lebanese subjects, 2008–2015: a cross-sectional study involving 10,814 subjects. Rheumatology international, (2016); 36(9): 1231-1236.
- Al-Mughales JA. Anti-Nuclear Antibodies Patterns in Patients With Systemic Lupus Erythematosus and Their Correlation With Other Diagnostic Immunological Parameters. Frontiers in Immunology, (2022); 13(2): 159-165.
- Nanda R, Gupta P, Patel S, Shah S, Mohapatra E. Uncommon antinuclear antibody patterns as diagnostic indicators. Clinical Biochemistry, (2021); 17(1): 9028-33.
- Hayashi N, Uto K, Imanishi A, Sugiyama D, Morinobu A, et al. Prevalence of anti-dense fine speckled 70 antibodies in healthy individuals and patients with antinuclear antibody-associated autoimmune rheumatic diseases in Japan. Medicine, (2021); 100(9): 219-234.
- Wei Q, Jiang Y, Xie J, Lv Q, Xie Y, et al. Analysis of antinuclear antibody titers and patterns by using HEp‐2 and primate liver tissue substrate indirect immunofluorescence assay in patients with systemic autoimmune rheumatic diseases. Journal of Clinical Laboratory Analysis, (2020); 34(12): e23546.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0