

Review Article
Role of Selective Cyclooxygenase-2 Inhibitors in Renal Colic Pain Reduction and Improvement: A Systematic Review of Clinical Trials
Mehdi Mohammadian Amiri1, Shaimaa Hameed Fayyadh2, Rosario Mireya Romero Parra3, Ali Hussein Demin Al-Khafaji4, Munther Abosaooda5, Mohammad Darvishi6*, Sepidehalsadat Emadichashmi7
Adv. life sci., vol. 9, no. 4, pp. 446-452, December 2022
*- Corresponding Author: Mohammad Darvishi (Email: darvishi1349 gmail.com)
Authors' Affiliations
2. Medical Laboratory Techniques Department, Al-maarif University College, Ramadi- Iraq
3. Universidad Continental, Lima- Perú
4. Techniques, Al-Mustaqbal University College, Babylon, Hillah- Iraq
5. College of pharmacy, the Islamic University, Najaf- Iraq
6. Tropical Medicine and Infectious Disease Department, AJA University of Medical Sciences, Tehran- Iran
7. Department of Anesthesia Medicine, School of Medicine, Babol University of Medical Sciences, Mazandaran- Iran
[Date Received: 12/09/2022: Date Revised: 27/11/2022; Date Published: 31/12/2022]
Abstract![]()
Introduction
Methods
Discussion
Conclusion
References
Abstract
Renal colic is an irritating condition that develops after obstruction of the ureter. Selective cyclooxygenase-2 inhibitors are types of non-steroidal anti-inflammatory drugs (NSAIDs) that have beneficial role in treatment various diseases. Hence, this systematic review summarizes the current knowledge about the role of selective cyclooxygenase-2 (COX-2) inhibitors as painkiller in renal colic pain management. The present systematic review was conducted according to the guidelines of the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) statements. Until September 2022, PubMed/Medline, Scopus, Web of Science, and Google Scholar databases were searched using the relevant keywords including “Selective Cyclooxygenase-2 Inhibitors”, “Parecoxib”, “Celecoxib”, “Rofecoxib”, “Renal Colic Pain” and “Ureteral Colic Pain”. Of 64 identified records through database searching, 6 randomized controlled trials (RCTs) were selected for this systematic review. The sample size in RCTs were between 53 and 338. The range of subject’s age was from 18 to 69. Overall, the evidence of this review revealed that the selective COX-2 inhibitors particularly celecoxib and parecoxib could alleviate renal colic pain in most of the studies through decreasing relevant pain score. Overall, selective COX-2 inhibitors seem to be effective in alleviating renal colic pain. However, further high quality assessments are required for demonstrating therapeutic role of selective COX-2 inhibitors against renal colic pain.
Keywords: Anti-Inflammatory Agents; Non-Steroidal; Renal Colic; Pain Management
Introduction![]()
Renal colic refers to painful and emergency conditions that occurs due to obstruction of the ureter [1,2]. Therefore, the term ureteral colic can describe this condition more accurately than renal colic. Renal colic manifests itself with high intensity and continuous pain. The renal colic pain originates from obstruction and distension of different parts of urinary system affected by stone including ureter, pelvicalyceal system, and renal capsule [1]. Renal colic is a prevalent condition in emergency departments that could involve people with an estimation as 1-15% during a lifetime. The prevalence of renal colic varies under the influence of various factors including age, sex, nationality, and geographical location [3]. Previous reports have estimated that renal colic appears in 240 per 100,000 persons [4,5]. Furthermore, statistics have indicated that the renal colic has higher incidence in men than women with a ratio of 3-2 to 1 [6]. Urinary calculi or urolithiasis or nephrolithiasis is recognized as the most important causative agent for development of renal colic pain [7]; however, several conditions such as lymphadenopathy, formation of blood clots caused by upper tract bleeding and sloughed renal papilla are other causes responsible for development of renal colic pain [1]. It has been documented that renal colic develops due to renal stones in 56% of cases [8]. It has been reported that approximately 600,000 patients with acute pain caused by renal calculi are annually admitted to the emergency departments in the United States which imposes a cost more than 2 billion dollars on the healthcare system [9]. Patients suffering from renal colic usually refer to the emergency departments with clinical manifestations such as severe loin pain, radiated pain to the flank, groin, and testes, nausea and vomiting [1,10]. Patients suffering from renal colic mention the pain caused by this disease as the worst pain they have ever experienced [11,12]. Renal failure, loss of kidney function and septicemia are serious and life threatening consequences of not treating renal colic on time. Hence, it is an emergency situation that requires quick management in the emergency departments [13]. Immediate admission to the hospital is considered as the main solution in the management of renal colic pain [14]. After diagnosis of renal colic with ultrasonography, radiography and computed tomography, therapeutic procedures such as surgery and medication can be effective in reducing pain [8,15]. Among these procedures, administration of analgesics including non-steroidal anti-inflammatory drugs (NSAIDs) or opioids is a regular procedure for pain relief; however, recently the administration of drugs such as alpha-blockers is recommended [11,16]. Cyclooxygenase-2 (COX-2) inhibitors are a class of NSAIDs which exert their therapeutic effects against various types of diseases including inflammatory diseases and cancer. They act through the inhibition of COX-2 as producer of prostanoids [17]. Hence, the present study reviews systematically the current knowledge about the role of selective COX-2 inhibitors as pain reliever drugs for renal colic pain management.
Methods![]()
Literature search and selection criteria
The present systematic review was carried out according to the guidelines of the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) statements.
Search Strategy
A systematic search was made on electronic databases, including Scopus, PubMed/Medline, Web of Science, and Google Scholar via keywords selected from Medical Subject Headings (MeSH). Selection of keywords was performed based on the PICO style (Participants, Intervention, Comparison, and Outcome). The following keywords: “Selective Cyclooxygenase-2 Inhibitors”, “Parecoxib”, “Celecoxib”, “Rofecoxib”, “Renal Colic Pain” and “Ureteral Colic Pain” were used for searching from databases. The search was done based on English language. The process of search was done by two authors, independently. In the current systematic review, the documents including dissertations, expert opinion and conference presentations was ignored due to imprecise results.
Eligibility Criteria
All relevant studies published until September 2022 were eligible in the current study. The present systematic review included all articles that evaluated the role of selective COX-2 inhibitors in renal colic pain management. Articles with insufficient information including case reports, observational studies, letters to the editor, reviews, conferences, and qualitative papers were not selected for this study.
Data Extraction
The literature was screened for extraction of required data by two investigators independently. The required data were used including name of drug (selective COX-2 inhibitors), administration route of drug, the dosage of the selective COX-2 inhibitors, study design, sample size, number of male patients, range of patient’s age, groups, pain measurement, the mean and SD of pain score before and after treatment with the selective COX-2 inhibitors, first author’s last name, country of origin and year of publication.
Quality Assessment
In order to evaluate the randomized controlled trials (RCTs) for their methodological quality, the Jadad scale was used. Based on Jadad scale, the score of each study varies from 0 to 5. The Jadad scale evaluate various items including randomization (Maximum points=2), blinding (Maximum points=2) and an account of all patients (Maximum points=1). The RCTs with maximum scores ≤2 was considered as low quality. On the other hand, the RCTs with minimum scores ≥3 was considered as high quality [18].
Study Characteristics
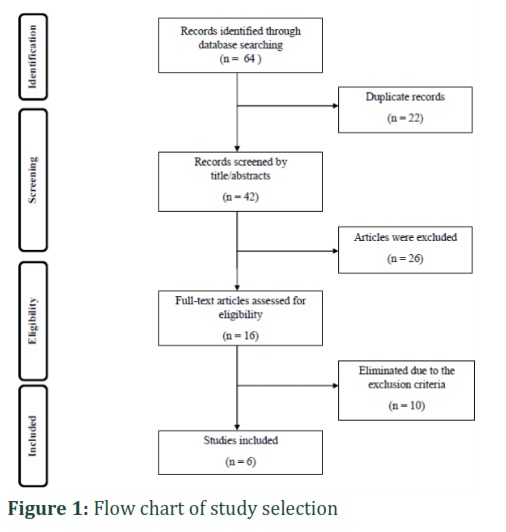
The process of study selection has been indicated in detail in Figure-1. After searching through mentioned databases, 64 studies were initially identified. There were 42 studies remaining after the removal of duplicates. Of these, 26 studies that did not have the inclusion criteria of the study were removed. Then, 16 scientific documents were chosen based on the research topic. Finally, 6 articles were included in the current systematic review after critical analysis. There were 6 RCTs included in final analyses. The sample size in RCTs was considered between 53 and 338. The range of subject’s age was from 18 to 69, representing that all patients were adult. All included publications were done after 2000. The included studies were performed in China with two studies [19,20], USA with one study [21], Switzerland with one study [22], Brazil with one study [23] and Kuwait with one study [24]. Table-1 summarizes the characteristics of the articles included in the current systematic review.
Quality Assessment
According to the Jadad scale for reporting the quality of RCTs, five studies had high quality (Maximum points ≤2) and only one study had low quality (Maximum points ≥3) (Table-2).
Several studies have evaluated the impact of the selective COX-2 inhibitors in renal colic pain management. However, the results of all of them are not reliable. In the present systematic review, we attempted to study the effectiveness of the selective COX-2 inhibitors as pain reliever drugs for reducing renal colic pain. The findings of this systematic review revealed that the selective COX-2 inhibitors drugs such as celecoxib, parecoxib and rofecoxib are useful medications in the alleviation of ureteric colic pain. Ureteric colic is recognized as one of regular urologic emergency conditions. The incidence (approximately 12%) and recurrence rate (50%) of this disease has become an important challenge in emergency departments. It has been reported that the subjects with ureteric colic experience an unbearable pain with high severity [11]. Hence, pain management is the first important step after admission of subjects suffering from ureteric colic to the emergency departments [25]. Some events such as ureteral obstruction, smooth muscle contraction of the ureter and subsequently inflammation have been shown to be associated to development of renal colic pain [26,27]. There are several pieces of evidence about the origin of renal colic pain. Ureteric colic pain develops because of obstruction of various parts of urinary system including ureter and pelvis. The obstruction of ureter because of renal calculi could induce pressure on the wall of urinary tract. Ureteral spasm has been proposed as another event which makes the renal colic pain worse [11,28]. On the other hand, several lines of evidence have demonstrated that pressure on the pelvis can induce the provoking, production and release of mediators of acute inflammation including prostaglandins [11,26]. Furthermore, it has been indicated that obstruction of the ureter due to kidney stones could induce inflammation in ureter because of the production and release of prostaglandins [11,27]. There is also an experiment by Nakada and colleagues that have reported up-regulation of COX-2 mRNA and protein levels as producer of prostaglandins during ureteral obstruction [29].
Excessive production of prostaglandins in response to injury caused by obstruction of the ureter due to nephrolithiasis is associated with renal colic pain with high severity [11]. To date, administration of NSAIDs, opioid and antispasmodics medications are used as a therapeutic solution to relieve severe pain induced by ureteric colic in emergency departments [25,26]. The findings of several trials have revealed that the efficiency and safety of NSAIDs in ureteric colic pain management. It has been exhibited that NSAIDs could relieve renal colic pain better than opioids [26,30]. Nowadays, NSAIDs have become a popular choice in emergency departments for controlling renal colic pain [19]. The mechanism of action of NSAIDs is inhibition of prostaglandin E2 secretion as a potent inflammatory mediator [25]. The production of prostaglandin E2 is affected by the activity of COX-2 which is inhibited by NSAIDs [31]. The COX-2 activity could inhibit by nonselective and selective inhibitors [32]. There are several reports about the therapeutic role of NSAIDs with nonselective COX-2 inhibition properties including ibuprofen, ketorolac [33], and indomethacin on renal colic [34]. Recently, the tendency to use selective COX-2 inhibitors has increased due to their effectiveness in alleviating various types of acute pain and safety [19]. In this regard, previous studies have been recommended that celecoxib and parecoxib as two important selective COX-2 inhibitors NSAIDs could alleviate different pains caused by surgery [35,36] and also renal colic [20,24]. Ureteral contractility is an important event in development of renal colic pain which lead to prostanoid release [11]. Jerde et al. showed that celecoxib could reduce ureteral contractility and prostanoid release in vitro because of inhibition of COX-2 with high specificity [37]. Furthermore, the role of parecoxib as an available selective COX-2 inhibitors NSAIDs has been investigated on contractility of ureters of the pig in vivo. The authors concluded that parecoxib plays role in decreasing the contractility of non-obstructed ureter in pig [38]. Tissue damage [39-47], especially kidney damage caused by diabetes [8-50] causes renal colic pain. Antioxidants can prevent tissue damage by affecting enzyme activities [51-54]. There are low publications about the therapeutic impact of selective COX-2 inhibitors on renal colic pain management. Hence, more scientific documents is needed to evaluate more precisely the efficacy of selective COX-2 inhibitors on ureteric colic treatment. The major strength of the current experiment was that it reviewed the impact of selective COX-2 inhibitors in renal colic pain control systematically for the first time. Our systematic review had some limitations such as the quality of included study, various subject populations, different methods of pain evaluation and the route of medication’s use as any other similar studies.
Figures & Tables


Taking together, selective COX-2 inhibitors particularly celecoxib and parecoxib could alleviate renal colic pain in most of the studies. The function of selective COX-2 inhibitors was better than conventional NSAIDs such as paracetamol and ketoprofen for management of renal colic pain through decreasing score of pain scale. Furthermore, toleration and safety of the selective COX-2 inhibitors were two important factors for choosing them in reducing ureteric colic pain. In conclusion, the present systematic review indicated that the selective COX-2 inhibitors can be administrate lonely or combined with more painkiller medications for ureteric colic pain management. Further RCTs are needed for demonstration of the effectiveness of selective COX-2 inhibitors in alleviating renal colic pain.
Author Contributions
Mehdi Mohammadian Amiri: monitoring of review, participation in data acquisition, interpretation of results, drafting of manuscript.
Mohammad Darvishi: Supervision of the review, writing and validation of the final version of the manuscript.
Shaimaa Hameed Fayyadh, Rosario Mireya Romero Parra, Ali Hussein Demin Al-Khafaji, Munther Abosaooda: Literature review, review analysis, validation of the final version of the manuscript.
The authors declare that there is no conflict of interest.![]()
References
- Bultitude M, Rees J. Management of renal colic. Bmj, (2012); 345e5499.
- Raja AS, Pourjabbar S, Ip IK, Baugh CW, Sodickson AD, et al. Impact of a health information technology–enabled appropriate use criterion on utilization of emergency department CT for renal colic. American Journal of Roentgenology, (2019); 212(1): 142-145.
- Torabi M, Shojaee F, Mirzaee M. Prevalence of Renal Colic in the Emergency Departments: A Multi-center Study. Hospital Practices and Research, (2021); 6(3): 123-126.
- Minotti B, Treglia G, Pascale M, Ceruti S, Cantini L, et al. Prevalence of microhematuria in renal colic and urolithiasis: a systematic review and meta-analysis. BMC urology, (2020); 20(1): 1-12.
- Tasian GE, Ross ME, Song L, Sas DJ, Keren R, et al. Annual incidence of nephrolithiasis among children and adults in South Carolina from 1997 to 2012. Clinical journal of the American Society of Nephrology, (2016); 11(3): 488-496.
- Scales Jr CD, Smith AC, Hanley JM, Saigal CS, Project UDiA. Prevalence of kidney stones in the United States. European urology, (2012); 62(1): 160-165.
- Brown J. Diagnostic and treatment patterns for renal colic in US emergency departments. International urology and nephrology, (2006); 38(1): 87-92.
- Azhar M, Kalwar MT, Akhtar N, Altaf A. Prevalence of acute renal colic presenting in emergency department of a tertiary care hospital. Rawal Medical Journal, (2022); 47(1): 152-152.
- Steinberg PL, Nangia AK, Curtis K. A standardized pain management protocol improves timeliness of analgesia among emergency department patients with renal colic. Quality Management in Healthcare, (2011); 20(1): 30-36.
- Thia I, Saluja M. An update on management of renal colic. Australian Journal of General Practice, (2021); 50(7): 445-449.
- Golzari SE, Soleimanpour H, Rahmani F, Mehr NZ, Safari S, et al. Therapeutic approaches for renal colic in the emergency department: a review article. Anesthesiology and pain medicine, (2014); 4(1).
- Holdgate A, Oh CM. Is there a role for antimuscarinics in renal colic? A randomized controlled trial. The Journal of urology, (2005); 174(2): 572-575.
- Mahamat MA, Diarra A, Kassogué A, Eyongeta D, Valentin V, et al. Renal colic: epidemiological, clinical etiological and therapeutic aspects at the urology department of the national reference general hospital of n’djamena (Chad). Open Journal of Urology, (2020); 10(02): 25.
- Kominsky HD, Rose J, Lehman A, Palettas M, Posid T, et al. Trends in acute pain management for renal colic in the emergency department at a tertiary care academic medical center. Journal of endourology, (2020); 34(11): 1195-1202.
- Dalziel PJ, Noble VE. Bedside ultrasound and the assessment of renal colic: a review. Emergency Medicine Journal, (2013); 30(1): 3-8.
- Payandemehr P, Jalili M, Mostafazadeh Davani B, Dehpour AR. Sublingual buprenorphine for acute renal colic pain management: a double-blind, randomized controlled trial. International journal of emergency medicine, (2014); 7(1): 1-5.
- Regulski M, Regulska K, Prukała W, Piotrowska H, Stanisz B, et al. COX-2 inhibitors: a novel strategy in the management of breast cancer. Drug discovery today, (2016); 21(4): 598-615.
- Gorabi AM, Abbasifard M, Imani D, Aslani S, Razi B, et al. Effect of curcumin on C‐reactive protein as a biomarker of systemic inflammation: An updated meta‐analysis of randomized controlled trials. Phytotherapy Research, (2022); 36(1): 85-97.
- Fu W, Yao J, Li Q, Wang Y, Wu X, et al. Efficacy and safety of parecoxib/phloroglucinol combination therapy versus parecoxib monotherapy for acute renal colic: a randomized, double-blind clinical trial. Cell biochemistry and biophysics, (2014); 69(1): 157-161.
- Lv JL, Tang QL. Comparative evaluation of efficacy of use of naftopidil and/or celecoxib for medical treatment of distal ureteral stones. Urolithiasis, (2014); 42(6): 541-547.
- Phillips E, Hinck B, Pedro R, Makhlouf A, Kriedberg C, et al. Celecoxib in the management of acute renal colic: a randomized controlled clinical trial. Urology, (2009); 74(5): 994-999.
- Engeler DS, Ackermann DK, Osterwalder JJ, Keel A, Schmid H-P. A double-blind, placebo controlled comparison of the morphine sparing effect of oral rofecoxib and diclofenac for acute renal colic. The Journal of urology, (2005); 174(3): 933-936.
- Glina S, Damiao R, Afif-Abdo J, Maria CFS, Novoa R, et al. Efficacy and safety of parecoxib in the treatment of acute renal colic: a randomized clinical trial. International braz j urol, (2011); 37697-705.
- Al-Terki A, Hussain J, El-Nahas AR, Aloumi A, Al-Asfoor M, et al. Parecoxib Vs Paracetamol for Treatment of Acute Renal Colic Due to Ureteric Calculi: A Randomized Controlled Trial. Urology, (2021); 14976-80.
- Jalili M, Entezari P, Doosti-Irani A, Masoomi R, Mirfazaelian H. Desmopressin effectiveness in renal colic pain management: Systematic review and meta-analysis. The American Journal of Emergency Medicine, (2016); 34(8): 1535-1541.
- Holdgate A, Pollock T. Systematic review of the relative efficacy of non-steroidal anti-inflammatory drugs and opioids in the treatment of acute renal colic. Bmj, (2004); 328(7453): 1401.
- Davenport K, Timoney AG, Keeley FX. Conventional and alternative methods for providing analgesia in renal colic. BJU international, (2005); 95(3): 297-300.
- Serinken M, Karcioglu O, Turkcuer I, Ozkan HI, Keysan MK, et al. Analysis of clinical and demographic characteristics of patients presenting with renal colic in the emergency department. BMC research notes, (2008); 1(1): 1-6.
- Nakada SY, Jerde TJ, Jacobson LM, Saban R, Bjorling DE, et al. Cyclooxygenase-2 expression is up-regulated in obstructed human ureter. The Journal of urology, (2002); 168(3): 1226-1229.
- Holdgate A, Pollock T. Nonsteroidal anti‐inflammatory drugs (NSAIDs) versus opioids for acute renal colic. Cochrane Database of Systematic Reviews, (2004); (1).
- Sander WJ, O'Neill HG, Pohl CH. Prostaglandin E2 as a modulator of viral infections. Frontiers in Physiology, (2017); 889.
- Zhu X-T, Chen L, Lin J-H. Selective COX-2 inhibitor versus non-selective COX-2 inhibitor for the prevention of heterotopic ossification after total hip arthroplasty: A meta-analysis. Medicine, (2018); 97(31).
- Forouzanfar MM, Mohammadi K, Hashemi B, Safari S. Comparison of intravenous ibuprofen with intravenous ketorolac in renal colic pain management; a clinical trial. Anesthesiology and pain medicine, (2019); 9(1).
- Jalili M, Shirani F, Entezari P, Hedayatshodeh M, Baigi V, et al. Desmopressin/indomethacin combination efficacy and safety in renal colic pain management: a randomized placebo controlled trial. The American Journal of Emergency Medicine, (2019); 37(6): 1009-1012.
- Faramarzi M, Roosta S, Eghbal MH, Nouri Rahmatabadi B, Faramarzi A, et al. Comparison of celecoxib and acetaminophen for pain relief in pediatric day case tonsillectomy: A randomized double‐blind study. Laryngoscope Investigative Otolaryngology, (2021); 6(6): 1307-1315.
- Li X, Zhou P, Li Z, Tang H, Zhai S. Intravenous Parecoxib for Pain Relief after Orthopedic Surgery: A Systematic Review and Meta-analysis. Pain and therapy, (2022); 1-17.
- Jerde TJ, Calamon-Dixon JL, Bjorling DE, Nakada SY. Celecoxib inhibits ureteral contractility and prostanoid release. Urology, (2005); 65(1): 185-190.
- Chaignat V, Danuser H, Stoffel MH, Z'Brun S, Studer U, et al. Effects of a non‐selective COX inhibitor and selective COX‐2 inhibitors on contractility of human and porcine ureters in vitro and in vivo. British journal of pharmacology, (2008); 154(6): 1297-1307.
- Gupta A, Gupta S, Mani R, Durgapal P, Goyal B, Rajput D, et al. Expression of Human epidermal growth factor receptor 2, Survivin, Enhancer of zeste homolog -2, Cyclooxygenase-2, p53 and p16 molecular markers in Gall bladder carcinoma. J Carcinog, (2021);20:7. DOI: 10.4103/jcar.JCar_4_21
- Gani IH, Al-Obaidi Z. Molecular docking studies of tyrosine kinase inhibitors: Exemplified protocol to advance pharmaceutical education in medicinal chemistry . Pharmacy Education, (2022). 22(4): 110–114. https://doi.org/10.46542/pe.2022.224.110114
- Mousa NO, Gado M, Osman A. Multimodality of human epidermal growth factor receptor-2 antagonism restores the apoptotic capacity of liver cancer cells. J Nat Sc Biol Med, (2020);11:118-27
- Rao S, Anthony ML, Chowdhury N, Kathrotia R, Mishra M, Naithani M, Sindhwani G, Singh N. Molecular characterization of lung carcinomas: A study on diagnostic, predictive, and prognostic markers using immunohistochemical analysis at a Tertiary Care Center in Uttarakhand, India. J Carcinog, (2021): 7;20:17. doi: 10.4103/jcar.jcar_14_21. PMID: 34729049; PMCID: PMC8531572.
- Simeon J, Thrush J, Bailey TA. Angiopoietin-like protein 4 is a chromatin-bound protein that enhances mammosphere formation in vitro and experimental triple-negative breast cancer brain and liver metastases in vivo. J Carcinog, (2021); 17: 20:8. doi: 10.4103/jcar.JCar_20_20. PMID: 34447288; PMCID: PMC8356708.
- Sowmya SV, Rao RS, Prasad K. Prediction of metastasis in oral squamous cell carcinoma through phenotypic evaluation and gene expression of E-cadherin, β-catenin, matrix metalloproteinase-2, and matrix metalloproteinase-9 biomarkers with clinical correlation. J Carcinog, (2020); 6;19:8. doi: 10.4103/jcar.JCar_8_20. PMID: 33033464; PMCID: PMC7511891.
- Gasmi A, Noor S, Piscopo S, Menzel A. Lifestyle Genetics-Based Reports in the Treatment of Obesity. Archives of Razi Institute, (2021);76(4):707.
- Shnewer Mahdi Al-Turfi Z, Al-Hadrawy S, Abadi Mohammed J, Chasib Jabal B. Evaluation of the Effect of Alcoholic Extract of Laurus Nobilis Leaves on Blood Biochemical Parameters and Histological Changes in the Liver and Kidney among Female Wistar Rats Treated with Depakene (Sodium Valproate). Archives of Razi Institute, (2022); 77(3), 981-989. doi: 10.22092/ari.2022.357272.2011
- Sharma G, Sharma SB. Synthetic Impatienol analogues as potential cyclooxygenase-2 inhibitors: a preliminary study. J. Appl. Organomet. Chem., (2021); 1(2), 66-75. doi:10.22034/jaoc.2021.276815.1006
- Alghamdi S, Asif M. Pyridazine derivatives act as phosphodiesterase-III, IV, and V Inhibitors. J. Appl. Organomet. Chem., (2021); 1(3), 116-124. doi:10.22034/jaoc.2021.289851.1024
- Darabi, H., Baradaran, A., Ebrahimpour, K. Subacute toxic effects of polyvinyl chloride microplastics (PVC-MPs) in juvenile common carp, Cyprinus carpio (Pisces: Cyprinidae). Caspian Journal of Environmental Sciences, (2022); 20(2): 233-242. doi: 10.22124/cjes.2022.5551
- Kaliwal, B. B., Ksheerasagar, R. L. Histological and Biochemical Changes in the Liver of Albino Mice on Exposure to Insecticide, Carbosulfan. Caspian Journal of Environmental Sciences, (2006); 4(1): 67-76.
- Beiranvand F, Alizadeh M. Plants for Remedies of Diabetes Mellitus in Iran. Plant Biotechnol Persa, (2019); 1 (1): 36-38.
- Urainab S, Mehreen A, Zahid S. Essential Oils Have the Potential to Be Effective Therapeutic Agents In The Future. Plant Biotechnol Persa, (2022); 4 (1):18-24.
- Abbasi N. Extraction and phytoanalysis of chemical compounds of Eucalyptus globulus leaf native to Dehloran, Ilam province, Iran by HS-SPME and GC-MS." Advances in Animal and Veterinary Sciences, (2020); 8(6): 647-652.
- Bahmani M, Jalilian A, Salimikia I, Shahsavari S, Abbasi N. Phytochemical screening of two Ilam native plants Ziziphus nummularia (Burm. f.) Wight & Arn. and Ziziphus spina-christi (Mill.) Georgi using HS-SPME and GC-MS spectroscopy. Plant Science Today, (2020); 6;7(2):275-80.
- Khademian amiri SA, Aghajanzadeh T, Jafari N, Mahmoudi M. Antioxidative compounds, enzymes activity and nutrient elements in Stachys byzantina are altered by climate conditions not by soil parameters. Caspian Journal of Environmental Sciences, (2022): 1-17.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0
![]()
![]()

