

Full Length Research Article
Neurokinin 1 receptor antagonist along with dexamethasone reduces the inflammation in COVID-19 patients: a novel therapeutic approach
Riffat Mehboob1,2*, Fridoon Jawad Ahmad3, Ahad Qayyum4, Muhammad Asim Rana4, Muhammad Akram Tariq5, Shadi Tamur6, Imran Shahid7, Iman M Mirza8, Amany Fathaddin9, Samy A Abusikkien10, Mohamed A Zayed11
Adv. life sci., vol. 10, no. 3, pp. 426-433, September 2023
*– Corresponding Author: Riffat Mehboob (mehboob.riffat@gmail.com)
Authors' Affiliations
2. RotoGen Biotech Pvt. Ltd., Lahore – Pakistan
3. Department of Genetics, University of Health Sciences, Lahore – Pakistan
4. Bahria International Hospital, Lahore – Pakistan
5. Higher Education Department (HED), Punjab, Lahore – Pakistan
6. Department of Pediatrics, College of Medicine, Taif University, Taif – Saudi Arabia
7. Department of Pharmacology and Toxicology, Faculty of Medicine, Umm Al-Qura University, Al-Abidiyah, P.O.Box 13578, Makkah – Saudi Arabia
8. Public Health and Community Medicine, Family and Community Medicine Department, Faculty of Medicine, University of Tabuk, Tabuk – Saudi Arabia
9. Pathology Department, College of Medicine, King Saud University, Riyadh – Saudi Arabia
10. Department of Anatomy, Faculty of Medicine, King Abdulaziz University, Rabigh, Saudi Arabia/Department of Anatomy, Ain Shams University, Cairo – Egypt
11. Department of Physiology, Faculty of Medicine, King Abdulaziz University, Rabigh – Saudi Arabia/ Department of Medical Physiology, Faculty of Medicine, Menoufia University – Egypt
[Date Received: 19/04/2023; Date Revised: 27/07/2023; Date Published Online: 30/09/2023; Date Updated: 06/09/2025]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background:
Corona virus infection is a respiratory infection, compromising the normal breathing in critical patients by damaging the lungs. The aim of this study was to evaluate the clinical outcomes of Substance P receptor Neurokinin 1 antagonist in COVID-19 patients against the usual treatments as controls.
Methods: It is a two-arm, open-label, randomized clinical trial that was carried out at Bahria International Hospital in Lahore, Pakistan. PCR-positive, hospitalized patients older than 18 years old, all sexes, and in the critical to life-threatening stage were included. 52 patients were placed in control group A and 67 patients were placed in intervention group B out of a total 119 patients who were randomly assigned to both arms. Before and after the intervention, lab tests were conducted in both groups. The control arm received standard therapy, while the intervention arm received standard therapy plus Aprepitant, a neurokinin-1 receptor antagonist. Additionally, both groups received oral administration of the corticosteroid dexamethasone.
Results: Patients in group A were on average 56.05 years old, compared to 58.1 years old in group B. There were 24 women in group A and 28 in group B, while Group A had 28 men and 24 women. Group A had three critical cases, but group B had five. The reduction in C-reactive protein in the intervention group, improvement in platelet count in group B, and normalization of ferritin and LDH levels in group B all indicated decreased inflammation in the biochemical and haematological parameters in both groups. However, because of the reduced sample size, it wasn't very significant.
Conclusion: The results of this recent trial provide a solid indication of Aprepitant's medicinal potential. Patients who got a combined therapy of dexamethasone and aprepitant had better clinical results, more favourable lab results, and lower levels of C-reactive protein, an inflammatory marker.
Keywords: Aprepitant; COVID-19 infection; Treatment; Dexamethasone; Neurokinin-1 receptor; Substance p; Trigeminal nerve
Introduction![]()
The COVID-19 novel coronavirus infection is currently pandemic. It is an acute respiratory and infectious illness for which there is no recognized cause or cure. It consistently results in losses of priceless lives and the global economy on a daily basis. Finding a treatment plan that involves creating a vaccine, creating a medication, or boosting the immune system is urgently needed. There is now no approved cure; instead, management and prevention methods for the spread of illness are prioritized. Various clinical trials are being conducted to assess the anti-viral and anti-inflammatory benefits of specific medications, but there are currently no conclusive results.
In response to nociception, the trigeminal nerve in the brainstem releases substance P (SP), which is a neurotransmitter and neuromodulator [1]. It is also the most prevalent neuropeptide in the airway [2]. The trachea is the primary route via which the coronavirus enters the body and travels to the lungs. These areas also experience non-neuronal cell releases of substance P (SP), such as immune cells. Additionally, nociception causes the trigeminal nerve to release it. By attaching to its receptor neurokin-1, substance P starts the cytokine storming, which results in the release of several inflammatory mediators. If Neurokinin-1 receptor antagonist decreases Substance P production, this may limit cytokine storming and, as a result, the respiratory tract’s hyperresponsiveness [3]. As with the COVID-19 infection, it might be directly related to the respiratory condition. It might be to blame for the disease's characteristic symptoms and elevated inflammation. The Neurokinin-1 Receptor (NK-1R) antagonist, aprepitant, must be used immediately to turn off the main switch. The SP's receptor, which controls how it works, is an NK-1R. Clinical symptoms of COVID-19 infection in the majority of complex cases included fever, coughing, exhaustion, muscle discomfort, sputum production, loss of smell, shortness of breath, joint pain, sore throat, headache, vomiting, and pink eyes. In extreme circumstances, it might cause organ failure, respiratory failure, and ultimately death.
The peripheral nervous system and the CNS both contain significant amounts of SP [4]. The soma of neurons is where SP is expressed. Large dense-core vesicles (LDCVs) are used to carry SP once it has been produced, and these vesicles exocytose to release the peptide either at axonal terminals or at the neuronal soma [5]. Immune cells like mast cells, macrophages, dendritic cells, T lymphocytes, neutrophils, and eosinophils can also release SP [6]. Substance P facilitates interactions between immune cells and neurons, with substance P derived from nerves influencing cytokine production and immune cell proliferation rates [7]. After being exocytosed, SP interacts with membrane-bound SP receptors that are either expressed on the same cell or on nearby cells. Neprilysin, a cell surface metalloendopeptidase, has the ability to break down unbound SP, suggesting that SP has a shorter half-life in tissues [8]. However, by interacting with fibronectin, SP can increase its half-life [9]. SP is said to be more stable in blood plasma, supporting this [10]. As a result, SP may join forces with additional molecules to extend the half-life of these molecules in blood or tissue.
A study was done to determine the part SP plays in human clinical cough. When compared to healthy controls, patients with persistent cough were shown to have higher serum SP levels. It was ascribed to asthmatic cough's airway sensitivity [11]. Previous studies from our own work have also revealed the involvement of SP and NK-1R in cardiorespiratory control [12], sleep wake cycle [12], inflammation [13] and involvement in fatal outcomes [14]. Some of our recent unpublished work also reports similar findings of SP/NK-1R involvement in inflammation, pain, pathologies, sudden deaths [15] etc. SP and NK-1R are also found to be involved in immunology [7,16], lung inflammation [2,7], respiratory network stability [17,18], heart failure [19] and neurological and psychiatric disorders [20]. An increased expression of SP in plasma of patients with other viral infections such as HIV and HSV is also well documented [6,21].
The inflammation that results from COVID-19 infection may be brought on by SP through the tachykinin receptor Neurokinin-1 (NK-1R). It might be the primary catalyst for the immune system's continued activation. If stopped, it might stop the chain reaction that leads to inflammation and, by extension, infection. Death from the virus is not brought on by the virus itself, but rather by cytokine storm-induced heart attack, organ failure, or respiratory failure. In a recent article, we suggested that the SP& NK/1R system might provide a neuropathological explanation for the low COVID-19 infection seen in infants and newborns [22].
A strong corticosteroid with anti-inflammatory and immunosuppressive effects is dexamethasone. It is frequently used to treat a number of ailments, such as inflammatory diseases, allergic reactions, and some forms of cancer. Corticosteroids are potent anti-inflammatory drugs frequently used in the treatment of a variety of illnesses. Examples include dexamethasone and methylprednisolone sodium succinate. Although corticosteroids can be quite successful, due to their potential side effects and the requirement for thorough monitoring, care should be taken when using them. Corticosteroids cause a variety of physiological effects by altering gene expression and binding to certain cell receptors. Corticosteroids can have both positive and negative effects in the context of illnesses of the central and peripheral nervous systems.
Sámano et al., conducted a study to examine the neuroprotective benefits of methylprednisolone in the in vitro treatment of acute spinal cord damage in rats [23]. The research revealed that the use of methylprednisolone decreased neuronal damage and enhanced functional recovery. This shows that in some neurological disorders, corticosteroids may have potential neuroprotective effects. It is crucial to remember that because of their potential negative effects, corticosteroids should only be used with caution. Hong et al., centred their systematic review and meta-analysis on the usage of methylprednisolone in COVID-19 patients [24]. Corticosteroids may be helpful in lowering mortality and the requirement for mechanical ventilation in serious instances, but the analysis indicated that they were also linked to an increased risk of secondary infections and other adverse effects. This emphasizes how carefully weighing the risks and benefits of using corticosteroids is essential, particularly when treating infectious disorders.
Regarding other therapeutic medications, riluzole and propofol are frequently utilized in various clinical contexts. A study by Kaur et al., (2016) investigated the neuroprotective effects of the general anaesthetic propofol against excitotoxic injury to the locomotor networks of the rat spinal cord in vitro [25]. The research discovered that administering propofol retained locomotor function and safeguarded against neural damage. Contrarily, riluzole is a medication used largely to treat amyotrophic lateral sclerosis (ALS). It has neuroprotective effects through regulating glutamate release and blocking voltage-gated sodium channels. Riluzole has been demonstrated to increase survival and reduce the progression of the disease in ALS patients, despite the fact that its exact mechanisms of action are still unclear. Inflammatory illnesses, including some neurological diseases, can be effectively treated with corticosteroids like methylprednisolone and dexamethasone.
Hence, we propose Aprepitant in combination with Dexamethasone for the treatment of COVID-19 infection. This is first clinical trial on this drug combination on COVID-19 patients. Aprepitant is used in combination with dexamethasone because they are both acting on the same pathway, NK-1R if blocked will not allow the binding of SP and corticosteroid, dexamethasone will act on neutral endopeptidase that will degrade SP.
Methods![]()
Trial Design and Participants
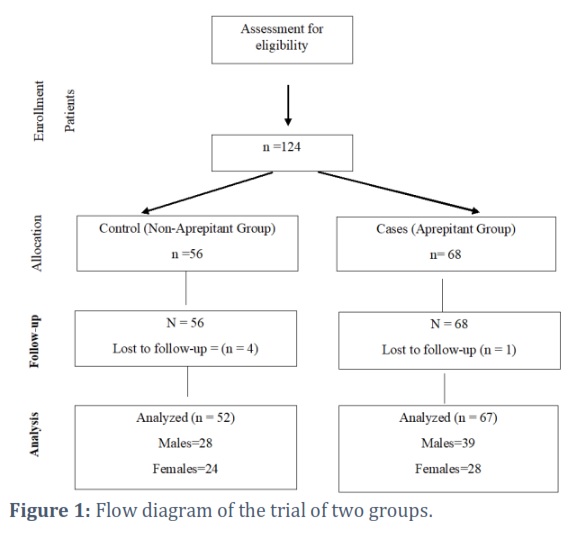
It is an open label, randomized clinical trial conducted at Bahria International Hospital, Lahore, to evaluate the effects of a combination therapy including Dexamethasone and Aprepitant in hospitalized patients with COVID-19. This trial is registered in clinicaltrials.gov (NCT04468646). The trial was conducted in accordance with the principles of the International Conference on Harmonization Good Clinical Practice guidelines and approved by the Bahria International Hospital Ethics Committee (IRB Approval from Bahria International Hospital, Lahore, No. 2/7/2020) and informed consent was obtained from the patients. 52 patients were enrolled in group A and 67 in group B (Figure 1, 2A).
Randomization
Case report form included demographics, major comorbidities, medication already being administered. Patients were divided randomly into two arms Control (A) receiving routine medication and Interventional (B) receiving Aprepitant as addition. Both the arms received routine management including Dexamethasone 20mg, but one arm received Aprepitant capsule 80mg once a day as an addition for 3-5 days depending on the condition of patient. Inclusion criteria was admitted patients above 18 years, both genders, lab confirmed COVID-19 positive based on PCR, more than 72 hours since the appearance of first symptoms. Patients with moderate to critical stages were included. Patients with respiratory diseases other than COVID-19 infection and pregnant females were excluded. Patients and care givers were not blinded to the allocated treatment. Lab investigations including total blood cell count, total leukocyte count, C-reactive protein, D-dimers, testing for lactate dehydrogenase was performed on daily basis to monitor the status of patient.
Primary Outcomes
Time to improvement on a 7-point ordinal scale as compared to baseline.
Secondary Outcomes
- Total in-hospital days and the total duration
- Treatment and prevention of inflammatory lung injury as measured by change in baseline of interleukin-6 (IL-6)
- Rate of Decline of COVID-19 viral load assessed by RT-PCR from nasopharyngeal samples
- Reduction from baseline of NRS for cough
- Reduction from baseline of NRS for nausea
- Time to normalization of fever for at least 48 hours
Results![]()
Patients
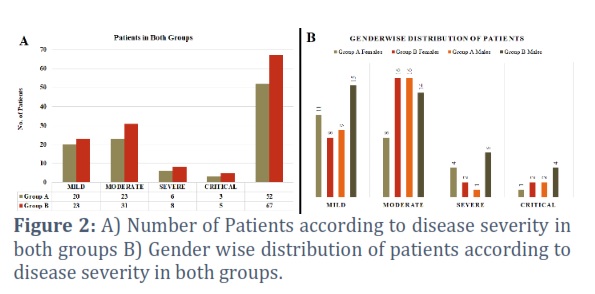
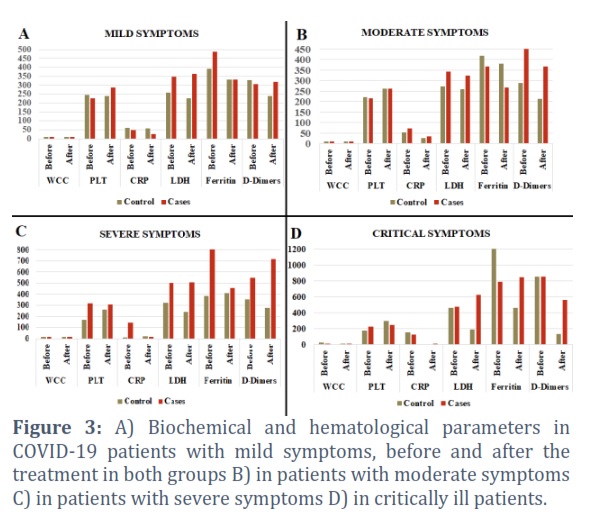
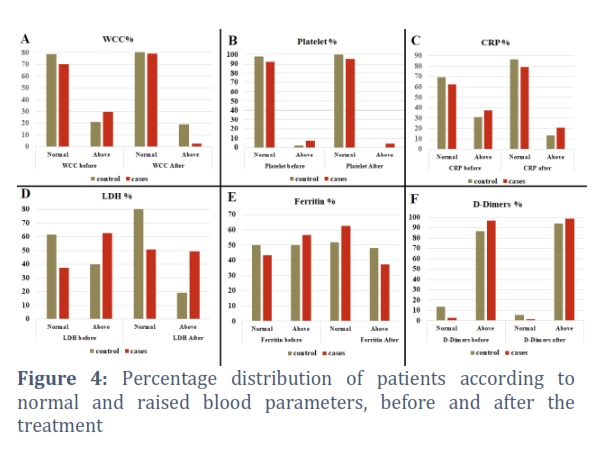
There were 52 patients in group A, 20 among these were mild, 23 moderate, 6 severe and 3 critical patients (Figure 2A) while 23 patients were mild, 31 moderate, 8 severe and 5 critical in group B, out of 67 patients (Figure 2A). Mean age of patients in the group A (Non-Aprepitant) was 56.05 years while 58.1 years in group B(Aprepitant)) (Table 1, 2). Group A had 28 males and 24 females while Group B had 39 males and 28 females (Figure 2 B, Table1,2). Group A: 20 mild, 23 moderate, 6 severe, 3 critical; Group B: 23 mild, 31 moderate, 8 severe, 5 critical. The mean white blood cell count (WCC) in group A and B at the beginning and after the treatment is indicated in table 1, Figure 3A-D, Figure 4A. The mean platelet count (PLT) in group A was 203.77×109/L before the treatment, 258.42 after the treatment while in group B was 247.75 before and 277.12×109/L after the intervention (Table 1,2, Figure 3A-D, Figure 4B). Apparently, there is not much difference in both the groups, however little improved in group B, but if we observe the individual patient data, we find much improvement in group B. The mean CRP in group A before the treatment was 70.55mg/L, after the treatment was 27.38 mg/L while in group B before the treatment was 98.3 mg/L and 21.57 mg/L after the treatment (Figure 3A-D, Figure 4C). The mean LDH levels in group A before the treatment was 328.15 units/L, 228.8 units/L after the treatment while in group B it was 419.8 units/L before and 455.4 units/L after the treatment (Table 1,2; Figure 3A-D, Figure 4D). The mean Ferritin levels in group A was 600 ng/mL before and 398.04 ng/mL after the treatment while in group B was 615.75 ng/mL before and 475.22 ng/mL after the treatment (Figure 3A-D, Figure E). The mean D-Dimers in group A was 457.67 mcg/mL before, 215.87 after the treatment while in group B it was 543.8 mcg/mL before and 491.7 mcg/mL after the intervention (Table 1,2; Figure 3A-D, Figure 4F).
Co-morbidities in group A and B included hypertension in 25 (48.01%) patients, diabetes in 21 (40.38%) patients. 43 (82.69%) patients had ischemic heart disease (IHD) in group A while hypertension in 43 (64.17%) patients, diabetes in 32 (47.76%) and IHD in 49 (73.13%) patients in group B. One critical patient out of 3 in group A had end stage renal disease and was on haemodialysis, one critical patient had immune thrombocytopenic purpura (ITP). Moderate patients had depression, asthma, obsessive compulsive disorder (OCD) and chronic obstructive pulmonary disease (COPD in one patient each. Azithromycin, Penitrax, Merosol, Remdisivir, Tocilizumab was administered in both the groups as routine management and usual care, irrespective of the group allocation. Clexane was used as anticoagulant in both groups. All the patients were discharged in both groups after recovery while 2 patients expired in group A and 1 in group B.
Figures & Tables


These initial findings show that a combination therapy of Dexamethasone and Aprepitant is effective in treating severe to critical COVID-19 patients [26]. Dexamethasone is a recently discovered drug for the treatment of critically ill COVID-19 patients. It is previously being used for similar indications such as post-surgery or post-chemotherapy emesis, nausea. Previously, it is in use alone as well as a combination therapy with Aprepitant. There are no major side-effects and safe for use in children as well as pregnant females. Rather it is used for lung maturation in premature labor and administered a day to week before delivery [27]. In our recent study, we have also suggested the similar role for Aprepitant [15]. It may also improve the respiratory conditions in premature labour as well as COVID-19 patients. We also suggest Ondansetron, a serotonin receptor antagonist along with these two drugs. This medication is already in use for the treatment of nausea and vomiting post chemotherapy. Serotonin is also involved with the nociceptive stimuli along with Substance P in inflammation. It may also be helpful in management of critically ill patients with respiratory problems as a result of COVID-19 infection.
Although mean of all the data is not showing much significant findings but a close look at the data of individual patients reveals a marked reduction in the levels of C-reactive protein in the intervention group B as compared to the group A. There were some confounding factors as well e.g., the medication that was given to both the groups including antibiotics, anticoagulants, Remdisivir and Tocilizumab, although it was given to both the groups. As the patients were randomly allocated to both the groups, coincidently, there were more aged patients in intervention group B and they had more co-morbidities. It may also affect the results.
SP secreted by the immune cells stimulates Th1 and Th17 autoreactive cells that migrate to the CNS and target nerves [28]. Hence, SP has been observed to be an important player in autoimmune responses. Expression of SP receptors, NK-1R is increased during inflammation, mainly on lymphocytes and macrophages. Hence, SP has a key role in immune system regulation by modulating the chemokines and adhesion molecules [7]. SP promotes angiogenesis by stimulating immune cells [29]. It affects the endothelial cells directly to produce nitric oxide or indirectly by interacting with mast cells and granulocytes [30].
Neutral endopeptidase (NEP) also known as Enkephalinase is SP degrading enzyme and animal studies have reported a decreased NEP activity in trachea of rats infected with parainfluenza virus type 1, corona virus and Mycoplasma pulmonis. NEP depletion in respiratory tract may lead to increased vulnerability to neurogenic inflammation by permitting larger concentrations of SP to reach NK-1R in the respiratory tract. This reduction of NEP activity elicits the pathological responses in respiratory infections [31]. Although SP is a neurotransmitter, but its exocrine role within the respiratory tract is well known [31]. Exogenous SP is involved in the mediation of inflammation in airways [29], causes smooth muscle contraction [30] and mucous secretion from tracheal glands [32] and increased vascular permeability [33]. Stimulation of sensory nerves by irritants including viruses causes bronchoconstriction [34] and also increases the attachment of neutrophils to the endothelium of venules [35], leading to inflammation. Several aspects of SP in airways are regulated by NEP [36]. So, it is already a proven fact that respiratory tract infections potentiate the vascular permeability produced by SP due to a decrease in NEP activity in the respiratory tract. The understanding of this mechanism is crucial in treatment of respiratory infections such as COVID-19. Alterations in NEP activity may result in altered SP concentrations in airways and leading to clinical manifestations of respiratory disease [31].
Small sample size (119 patients, 52 in group A, 67 in group B). Age and gender matched cases and controls were not present as there was random and convenient sampling. Only medical records and biochemical parameters are included in this study. Very few severe and critical patients were enrolled in study, most of the patients were with mild to moderate symptoms but all the patients showed improvement and recovery. These are all limitations of the study.
The positive and encouraging fact is that this is the only Phase III study so far as far as the effectiveness of Neurokinin-1 Receptor antagonist on COVID-19 is concerned. We have all the theoretical and experimental evidence to claim the effectiveness of NK-1 Receptor antagonist on respiratory recovery on COVID-19 patients. This pilot study has also shown effectiveness in individual patient data; however, no significant values are obtained due to small sample and confounding factors. Furthermore, this drug is already available, cost-effective and FDA approved. It has no adverse effects. All the patients were recovered and discharged except 2 mortalities in group A and 1 in group B but was attributed to comorbidities.
There is an urgent need to extend this trial on more patients and in different populations to have significant findings and confirmation. Inflammatory markers such as Interleukin-6, TNF-α and Interleukin- α should be investigated by real time PCR (Before and after the intervention). Substance P and NK-1R ELISA should be conducted on plasma of patients before and after the intervention. Pharmacokinetic studies should also be conducted. Hence, dexamethasone, a corticosteroid may modulate immune-mediated lung injury and reduces the progression to respiratory failure and death by mainly affecting the NEP and Aprepitant may block the receptor of SP. Both dexamethasone and Aprepitant are affecting the SP, one by potentiating the SP degrading enzyme and the other by antagonizing the SP receptor, therefore, reducing the SP binding the receptor. So, the limitation of this study is small sample size as the number of patients decreased in Pakistan and we couldn’t enrol more patients. Here, we suggest, to conduct this trial in other populations where there is still surge of COVID-19 and ruling out the confounding variables. But this study gives a strong clue for the effectiveness of this treatment for severe to critical COVID-19 patients.
Drugs like Dexamethasone and Aprepitant were previously prescribed for different conditions like nausea and emesis following surgery or chemotherapy. The study highlights the benefits of repurposing current medications to meet new medical issues by demonstrating their promise in treating COVID-19. Dexamethasone and Aprepitant are regarded as safe for usage in both pregnant women and children due to their well-known safety profiles. This finding is significant because it raises the possibility that a variety of people, including those with specific medical issues, may benefit from the suggested combination medication. The study suggests that additional clinical studies are necessary to confirm the efficacy of the combination medication in a wider patient group. The ability to draw firm conclusions is constrained by the small sample size and confounding variables. Stronger proof would be produced by conducting more thorough trials with greater sample sizes and controlled conditions.
WCC count decreased after the intervention. Platelet count improved, CRP levels reduced to normal in most of the patients in intervention group. Much improvement in Ferritin levels in group B and they were reduced to normal. Improvement in LDH levels but not statistically significant. D-Dimers remain raised in most of the cases in both groups. Substance P (SP) is a possible cause of the initiation of cytokine storming developed in Covid-19 infection and we suggest Neurokinin-1 Receptor antagonist, Aprepitant, as a drug to be used for its treatment. It may help in the management of cytokine storming as well as improving the respiratory outcome in severe to critical patients.
Competing Interest
The authors declare no conflict of interest.
Author Declarations
I confirm all relevant ethical guidelines have been followed, and any necessary IRB and/or ethics committee approvals have been obtained. The details of the IRB/oversight body that provided approval or exemption for the research described are given below: The trial was conducted in accordance with the principles of the International Conference on Harmonization Good Clinical Practice guidelines and approved by the Bahria International Hospital Ethic Committee. All necessary patient/participant consent has been obtained and the appropriate institutional forms have been archived. I understand that all clinical trials and any other prospective interventional studies must be registered with an ICMJE-approved registry, such as ClinicalTrials.gov. I confirm that any such study reported in the manuscript has been registered and the trial registration ID is provided (ClinicalTrials.gov Identifier: NCT04468646).
RM conceived the idea, planned and designed the study. FJA facilitated this study and critically analysed the whole work. AQ, MAR and MAT conducted the clinical trial, EF, IMM and MAZ provided their expertise in clinical aspects. All the authors have contributed in writeup and finalization
![]()
References
- Khan MA, Ho Y-S. Arsenic in drinking water: a review on Jia W, Wang W, Li R, Zhou Q, Qu Y, et al. Effect of Qinbai Qingfei Concentrated Pellets on substance P and neutral endopeptidase of rats with post-infectious cough. BMC Complementary Medicine and Therapies, (2020); 201-10.
- Li M, Shang Y-x. Neurokinin-1 receptor antagonist decreases [Ca2+] i in airway smooth muscle cells by reducing the reverse-mode Na+/Ca2+ exchanger current. Peptides, (2019); 11569-74.
- Mehboob R, Kurdi M, Bamaga A, Aldardeir N, Nasief H, Moshref LH, Alsinani T, Rayes AO, Jabbad RH. Substance P/ Neurokinin-1 Receptor, Trigeminal Ganglion, Latency, and Coronavirus Infection-Is There Any Link? Front Med (Lausanne). (2021); 18;8:727593.
- Hökfelt T, Vincent S, Dalsgaard C, Skirboll L, Johansson O, et al. Distribution of substance P in brain and periphery and its possible role as a co-transmitter; 1982. pp. 84-106.
- De Camilli P, Jahn R. Pathways to regulated exocytosis in neurons. Annual review of physiology, (1990); 52(1): 625-645.
- Suvas S. Role of substance P neuropeptide in inflammation, wound healing, and tissue homeostasis. The Journal of Immunology, (2017); 199(5): 1543-1552.
- Mashaghi A, Marmalidou A, Tehrani M, Grace PM, Pothoulakis C, et al. Neuropeptide substance P and the immune response. Cellular and molecular life sciences, (2016); 734249-4264.
- Erdös EG, Skidgel RA. Neutral endopeptidase 24.11 (enkephalinase) and related regulators of peptide hormones 1. The FASEB journal, (1989); 3(2): 145-151.
- Rameshwar P, Oh H, Yook C, Gascon P, Chang V. Substance p-fibronectin-cytokine interactions in myeloproliferative disorders with bone marrow fibrosis. Acta haematologica, (2002); 109(1): 1-10.
- Corbally N, Powell D, Tipton KF. The binding of endogenous and exogenous substance-P in human plasma. Biochemical pharmacology, (1990); 39(7): 1161-1166.
- Otsuka K, Niimi A, Matsumoto H, Ito I, Yamaguchi M, et al. Plasma substance P levels in patients with persistent cough. Respiration, (2011); 82(5): 431-438.
- Lavezzi AM, Mehboob R, Matturri L. Developmental alterations of the spinal trigeminal nucleus disclosed by substance P immunohistochemistry in fetal and infant sudden unexplained deaths. Neuropathology, (2011); 31(4): 405-413.
- Mehboob R, Tanvir I, Warraich RA, Perveen S, Yasmeen S, et al. Role of neurotransmitter Substance P in progression of oral squamous cell carcinoma. Pathology-Research and Practice, (2015); 211(3): 203-207.
- Mehboob R. Substance P/Neurokinin 1 and Trigeminal System: A Possible Link to the Pathogenesis in Sudden Perinatal Deaths. Front Neurol, (2017); 8:82.
- Alwazzan A, Mehboob R, Hassan A, Perveen S, Sadaf, et al. Elevated neurokinin-1 receptor expression in uterine products of conception is associated with first trimester miscarriages. Frontiers in Physiology, (2020); 11554766.
- Pakai E, Tekus V, Zsiboras C, Rumbus Z, Olah E, Keringer P, Khidhir N, Matics R, Deres L, Ordog K, Szentes N, Pohoczky K, Kemeny A, Hegyi P, Pinter E, Garami A. The Neurokinin-1 Receptor Contributes to the Early Phase of Lipopolysaccharide-Induced Fever via Stimulation of Peripheral Cyclooxygenase-2 Protein Expression in Mice. Front Immunol, (2018);9:166.
- Szereda-Przestaszewska M, Kaczyńska K. Serotonin and substance P: Synergy or competition in the control of breathing. Auton Neurosci, (2020);225:102658.
- Yeh S-Y, Huang W-H, Wang W, Ward CS, Chao ES, et al. Respiratory network stability and modulatory response to substance P require Nalcn. Neuron, (2017); 94(2): 294-303. e294.
- Dehlin HM, Levick SP. Substance P in heart failure: the good and the bad. International journal of cardiology, (2014); 170(3): 270-277.
- Iftikhar K, Siddiq A, Baig SG, Zehra S. Substance P: A neuropeptide involved in the psychopathology of anxiety disorders. Neuropeptides, (2020); 79101993.
- Douglas SD, Ho W-Z, Gettes DR, Cnaan A, Zhao H, et al. Elevated substance P levels in HIV-infected men. Aids, (2001); 15(15): 2043-2045.
- Mehboob R, Lavezzi AM. Neuropathological explanation of minimal COVID-19 infection rate in newborns, infants and children – a mystery so far. New insight into the role of Substance P. J Neurol Sci, (2021);420:117276.
- Sámano C, Kaur J, Nistri A. A study of methylprednisolone neuroprotection against acute injury to the rat spinal cord in vitro. Neuroscience, (2016); 315136-149.
- Hong S, Wang H, Zhang Z, Qiao L. The roles of methylprednisolone treatment in patients with COVID-19: A systematic review and meta-analysis. Steroids, (2022); 183109022.
- Kaur J, Flores Gutiérrez J, Nistri A. Neuroprotective effect of propofol against excitotoxic injury to locomotor networks of the rat spinal cord in vitro. European Journal of Neuroscience, (2016); 44(7): 2418-2430.
- Mehboob R, Ahmad FJ, Qayyum A, Rana MA, Gilani SA, et al. Aprepitant as a combinant with Dexamethasone reduces the inflammation via Neurokinin 1 Receptor Antagonism in severe to critical Covid-19 patients and potentiates respiratory recovery: A novel therapeutic approach. MedRxiv, (2020); 2020.2008. 2001.20166678. https://www.medrxiv.org/content/10.1101/2020.08.01.20166678v3.article-metrics
- Vilisaar J, Kawabe K, Braitch M, Aram J, Furtun Y, et al. Reciprocal regulation of substance P and IL-12/IL-23 and the associated cytokines, IFNγ/IL-17: A perspective on the relevance of this interaction to multiple sclerosis. Journal of Neuroimmune Pharmacology, (2015); 10457-467.
- Ziche M, Morbidelli L, Pacini M, Geppetti P, Alessandri G, et al. Substance P stimulates neovascularization in vivo and proliferation of cultured endothelial cells. Microvascular research, (1990); 40(2): 264-278.
- Ziche M, Morbidelli L, Masini E, Amerini S, Granger HJ, et al. Nitric oxide mediates angiogenesis in vivo and endothelial cell growth and migration in vitro promoted by substance P. The Journal of clinical investigation, (1994); 94(5): 2036-2044.
- Lundberg J, Hökfelt T, Martling C-R, Saria A, Cuello C. Substance P-immunoreactive sensory nerves in the lower respiratory tract of various mammals including man. Cell and tissue research, (1984); 235251-261.
- Borson D, Brokaw J, Sekizawa K, McDonald D, Nadel J. Neutral endopeptidase and neurogenic inflammation in rats with respiratory infections. Journal of Applied Physiology, (1989); 66(6): 2653-2658.
- Sekizawa K, Tamaoki J, Nadel J, Borson D. Enkephalinase inhibitor potentiates substance P-and electrically induced contraction in ferret trachea. Journal of Applied Physiology, (1987); 63(4): 1401-1405.
- Baker AP, Hillegass LM, Holden DA, Smith WJ. Effect of kallidin, substance P, and other basic polypeptides on the production of respiratory macromolecules. American Review of Respiratory Disease, (1977); 115(5): 811-817.
- Lundberg J, Saria A, Brodin E, Rosell S, Folkers K. A substance P antagonist inhibits vagally induced increase in vascular permeability and bronchial smooth muscle contraction in the guinea pig. Proceedings of the National Academy of Sciences, (1983); 80(4): 1120-1124.
- Sellick H, Widdicombe J. Stimulation of lung irritant receptors by cigarette smoke, carbon dust, and histamine aerosol. Journal of applied physiology, (1971); 31(1): 15-19.
- Wang FL, Zhang GT, Zhou YN, Yang XX, Zhou L, et al. The expanded effects of sevoflurane on the nervous system: the harmful effect of residual concentration of sevoflurane on the respiratory system through neurogenic inflammation. Ibrain, (2021); 7(2): 68-79.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0