

Review Article
An updated review on anti-diabetic agents and their functions: a comparative study
Abrar Hussain1, Abdul Latif2, Zainia Rehmat3, Musarat Riaz4, Nelofer Jamil4, Muhammad Amir1,5, Muhammad Asif1,6
Adv. life sci., vol. 10, no. 3, pp. 326-334, September 2023
*– Corresponding Author: Muhammad Asif (asifjallali@yahoo.com )
Authors' Affiliations
2. Department of Microbiology, BUITEMS, Quetta – Pakistan
3. Department of Biotechnology, Sardar Bahadur Khan Women's University Quetta – Pakistan
4. Department of Chemistry, Sardar Bahadur Khan Women's University Quetta – Pakistan
5. CASVAB, University of Balochistan, Quetta – Pakistan
6. Office of Research Innovation and Commercialization, BUITEMS, Quetta – Pakistan
[Date Received: 01/12/2022; Date Revised: 22/05/2023; Date Published Online: 30/09/2023; Date Updated: 06/09/2025]
Abstract![]()
Introduction
Methods
Discussion
Conclusion
References
Abstract
Keywords: Diabetes mellitus; Sulfonylureas; Thiazolidinediones
Introduction![]()
Diabetes mellitus (DM) is a collection of metabolic diseases characterized by hyperglycemia, in which a person does not yield adequate insulin, or the body cells did not respond conscientiously to insulin that is formed [1]. Diabetes is a Greek term meaning “to pass through” suggesting signs of polydipsia, polyuria, and polyphagia, while mellitus is the Latin word meaning “sweetened” proposing glycosuria [2].
Diabetes mellitus usually has been distributed and deal with a number of aspects but the most common three types are: (i) Type 1 diabetes mellitus (T1DM) is as well designated “juvenile diabetes” in which the body becomes unable to harvest insulin also known as insulin-dependent diabetes mellitus (IDDM). (ii) Type 2 diabetes mellitus (T2DM) state in which an insulin utilizing cells fails to respond appropriately this sort mentioned to “adult-onset diabetes” and is non-insulin-dependent diabetes mellitus (NIDDM). (iii) This kind of diabetes commonly occurs in women during her pregnancy and may proceed to T2DM without any history of diabetes known as gestational diabetes [3,4].
In addition, many other varieties of diabetes including exogenous pancreatic disease, monogenetic diabetes syndrome, chemically or drug induced, endocrine diabetic disorder, and diabetes related to infection [5]. Worldwide T1DM is more predominant among children in particular between the ages of (10-14) years [6]. The strongest risk factor for T1DM progression is genetics. In contrast, approximately 25% of individuals who have a family history of diabetes exhibit T2DM, which is more prevalent in adults [7-9].
Clinically, diabetes mellitus is characterized by a high plasma glucose level, weight loss, polyuria, eyesight impairment, and polydipsia while chronic hyperglycemia prominently led to growth retardation and more susceptible to infections [10]. Diabetes can harm blood vessels, nerves, eyes, and kidneys, which can cause many problems. People with diabetes are much more likely to develop heart disease than those without it [11]. Diabetes is a debilitating chronic illness linked to reduced life expectancy, quality of life, and economic costs for patients and society due to healthcare, medications, and early death [12].
Moreover, diabetes has been considered the highest 21st century challenging health distress, with an estimated 285 million individuals affected worldwide in 2010. The incidence of diabetes is expected to increase by more than 20% in adults and up to 69% in seniors in developing countries over the next two decades [13-15]. By 2030, it is expected that over 400 million individuals worldwide will have type 2 diabetes mellitus, including young people living in regions with low- or middle-income [16].
Insulin injections are necessary to control T1DM, while T2DM is managed using insulin-containing or non-insulin-containing drugs. Oral medicines and insulin can cause low blood sugar. Studies have also addressed the use of current pharmaceuticals, alternative treatments, and activity management therapy [17,18]. Various oral insulin secretagogues are currently available for treating type II diabetes mellitus, including Sulfonylureas, biguanides, repaglinide, thiazolidinediones, nateglinide, insulin, pramlintide, alpha-glucosidase inhibitors, and exenatide [19].
These medications work differently, for example, by stimulating insulin secretion, inhibiting hepatic gluconeogenesis, or increasing insulin receptor sensitivity [20]. Personalized medicine advancements have resulted in discovering polymorphisms that affect drug-metabolizing enzymes, drug carriers, targets, and receptors [21]. Therefore, the goal of the present assessment is to learn more specifically pertaining to diabetes mellitus, including its clinical manifestation, statistics on incidence, negative consequences, and treatment regime at present.
Methods![]()
Literature search strategy and selection criteria
We looked into the adherence and compliance of patients with regard to diabetes, hypoglycemic agents, insulin, prescription administration and psychological aspects. We examined a variety of factors, such as administration, unfavorable effects, and diabetic treatment care. We thoroughly looked at several databases, notably Google Scholar, PubMed, and several others to find pertinent material. In order to find relevant material, we searched for these databases from their origin until October 2022. Also, we looked over the bibliographies of each disclose that was acquired and looked for pertinent articles in the fields.
Figures & Tables
Discussion![]()
Epidemiology
The prevalence of diabetes is increasing worldwide, with more than 80% of adult cases expected to occur in newly established or developing nations by 2030, resulting in a projected total of 438 million cases [22]. As a result of this trend, a growing number of individuals are experiencing significant complications affecting the cardiovascular system, kidneys, eyes, and peripheral nerves. The rise in incidence has also been documented among children and young adults, where T2DM may currently exceed T1DM [23]
In Japan, the incidence of (T2DM) has shown an alarming increase among junior high school students, rising from (7.3/100,000) between (1976-1980) to (13.9/100,000) in (1991–1995) respectively, with T2DM occurrences surpassing those of T1DM [24]. In cats, male gender has been identified as a common risk factor in the disease progression, with several risk factors in common with T2DM in humans, such as aging, lack of physical activity, and obesity [25]. In 2002, DM was reported as the sixth leading cause of death, accounting for millions of deaths [26].
The genetic predisposition accounts for 70-75% of susceptibility to T1D, with lifestyle factors also playing a role in triggering beta cell loss and diabetes onset. While, T1D prevalence in children aged 0-14 years varies significantly between different countries, with Finland, Sweden, and Norway ranked highest at 57.6, 43.1, and 32.8 cases per 100,000 annually [27-29].
Furthermore, global prevalence of T2D has risen significantly, with the number of affected individuals in 2000 rising commencing (151 to 415 million) presently [30]. In the context of Pakistan, a prior investigation conducted in the Sindh province showed a prevalence rate of 13.9% [31].
Pathophysiology of diabetes
T1DM is a complex immunological illness develops through a combination of immunologic as well as genetic factors [32]. Obesity is a major factor in the development of T2DM as it causes resistance in peripheral tissues and inflammation in metabolic-activated adipose tissue, making it a significant genetic and environmental factor in T2DM development [33]. Reactive oxygen species (ROS) generation is an essential factor in the pathophysiology of macro- and micro-vascular complications related to diabetes, including diabetic nephropathy [34]. Insulin resistance, glucose, free fatty acids (FFA) are linked to increased ROS production and, as a result, oxidative stress, which can impair insulin secretion and efficiency and accelerate the progression to overt T2DM [35]. According to Randle’s hypothesis from over three decades ago, FFA and glucose compete for the primary energy source in the heart muscles, resulting in reduced glucose oxidation during high FFA levels [36].
In recent years, researchers have identified a link between T2D and oxidative stress-induced inflammation. Oxidative stress happens when the body can’t handle the production of harmful reactive oxygen species. In T2D, there is often increased mitochondrial uncoupling and beta-oxidation, which can lead to higher ROS production. This increased ROS generation can activate inflammatory pathways, leading to a cascade of stress pathways that negatively impact insulin signaling [37,38].
Lipid peroxidation is when lipids are broken down by reactive oxygen species (ROS), which can cause damage to tissue and inflammation. In diabetic patients, high levels of iso-prostane indicate increased lipid peroxidation and can lead to complications. Antioxidants like catalase, glutathione peroxidase, and superoxide dismutase are important for neutralizing ROS and preventing oxidative stress. Diabetic patients with lower or high levels of antioxidants may experience increased ROS generation and complications. The beta islet, which produces insulin, is especially vulnerable to damage because of its low antioxidant defenses [39-41]. The beta islet, which produces insulin, is particularly susceptible to oxidative stress-induced damage due to its low innate antioxidant defenses. Therefore, maintaining a healthy antioxidant status may be essential in protecting against diabetic complications [42]. High blood sugar levels, or hyperglycemia, have recently been linked to the initiation of surplus biochemical pathways, such as stress-activated signaling pathways like nuclear factor-kB (NF-kB), NH2-terminal Jun kinases (JNK)/stress-activated protein kinases (SAPK), p38 mitogen-activated protein (MAP) kinase, and hexosamine. These pathways can lead to oxidative stress, which is caused by NADH-induced reductive stress [43]. Reducing hyperglycemia-induced reductive stress may provide therapeutic options for treating diabetes and its complications [44].
Metabolic diseases, especially diabetes, can be caused by errors in the signaling pathways of IRS-1 and IRS-2 proteins. IRS proteins help regulate glucose absorption, lipogenesis, protein synthesis, and cell viability [45]. Mice with IRS-1 deficiency have hypersecretion of insulin as compensation, while IRS-2 alteration promotes hyperglycemia and can be fatal. IRS-3 and IRS-4 don’t show observable phenotypes, but IRS-4 acts as an insignificant function in growth, reproduction, and glucose homeostasis. Insulin resistance in IRS2–/– mice is due to deregulated PI3K activity. Mutations in the GCG-R gene may contribute to T2D in the French population [46], and the significance of Gly972Arg and Ala513Pro variations in the IRS-1 gene in the development of NIDDM is unclear. Glycogen regulates hepatic glucose production and helps regulate glucose homeostasis [47,48].
Medication for diabetes
Biguanides
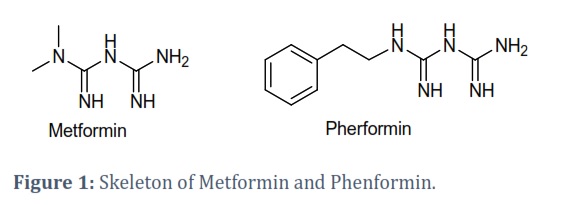
Metformin hydrochloride (biguanide) is a "first-line therapy" that is widely used to lower blood glucose level in person who have newly been established T2DM. Unlike other synthetic medications, metformin is derived from a natural substance used as part of a natural remedy and was not designed to target a specific route or disease [49]. It is particularly useful in overweight and obese individuals because it inhibits the production of glucose by the liver, increases insulin sensitivity, and improves glucose uptake by phosphorylating insulin [50].
The medication is chemically constituted of two guanidine groups linked together by the removal of ammonia, making it a member of the biguanide class of medications. Metformin is available in oral formulations ranging from 500 mg/b.i.d. or t.i.d. to a maximum of 2,550 mg/day (roughly 35 mg/kg/day), with 2,000 mg/day being a commonly recommended maximum in some guidelines. Studies have shown that metformin reduces fasting plasma glucose levels by 1.1 mmol/L and HbA1c by 0.9%. At a dosage of 2000 mg, the comparable declines were 4.3 mmol/L and 2.0% (21.9 mmol/mol; p < 0.01) [51,52]. Orally administrated metformin have been absorbed almost 70% by the small-intestine, while, remaining of the drug passed into colon and eliminated in feces. However, metformin is not recommended for individuals with high blood creatinine levels (1.5 mg/dL in men and 1.4 mg/dL in women) or those with renal function at risk [53].
Recent studies of metformin have shown an extraordinary concentration in gastrointestinal tract, kidneys, liver and bladder imitating the route of action by positron emission tomography (PET) also a slight agglomeration in muscle tissues [54]. The medication lowers intestinal glucose absorption as well as LDL and VLDL. A reduction in triglycerides and free fatty acids suggests that the medication has a cardio-protective effect and is likely to help improve insulin sensitivity [55]. Metformin lowers glucose production in the liver by suppressing a process called gluconeogenesis. It does this by activating a protein called AMP-activated protein kinase while inhibiting a part of the mitochondrial respiratory chain complex 1, increasing NADH oxidation and ultimately reducing ATP synthesis [52]. Studies have shown that metformin also has an effect on cellular proliferation and inflammation. It has been found to suppress proliferation in keratinocytes via the mitogen-activated protein kinase pathway and reduce proliferative and proinflammatory cytokines in cultured human keratinocytes via the mammalian target of rapamycin signaling pathway [56,57]. Figure 1 represents the structures of Metformin and Phenformin.
Sulfonylureas
Sulfonylurea (SU) skeleton-containing substances are one of the most prominent organic compounds displaying promising anti-diabetic properties among their other pharmacological functions [58]. If a patient is unable to take metformin, another oral anti-diabetic drug, such as sulfonylurea, may be administered. The justification for metformin prescribing as the primary-treatment for T2DM relies entirely on its apparent good effect on traditional surrogate outcomes [59]. Tolbutamide was the first SU agent, and it was introduced in Germany during the 1950. Glimepiride, the second SU agent, which is generally alluded to as a third-generation agent, was launched in 1995 [60]. In individuals with noninsulin-dependent diabetes mellitus, glipizide, a second-generation sulfonylurea, offers a significant anti-diabetic effect [61].
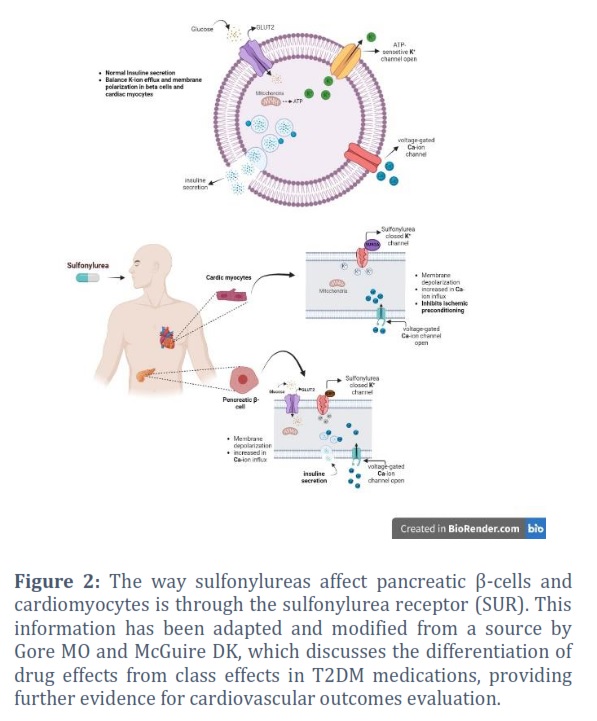
Second- and third-generation sulfonylureas are chosen based on perceived higher efficacy and safety characteristics. Sulfonylureas are still a popular choice for treating diabetes, either on their own or with another drug. They account for about 25% of newly started diabetes treatment [62]. Sulfonylureas lower glucose levels by increasing insulin release from the pancreas and inhibiting the production of glucose in the liver. This is done by blocking KATP channels [63]. Elderly people with DM treated with sulphonylureas had a 36% greater risk of hypoglycemia than younger people. SUs are the preferred therapeutic agents in diseases such as neonatal diabetes, MODY-3(HNF-1) mutations, and certain Transcription Factor 7-like 2 polymorphisms [64]. KATP channels are found in a kind of tissues, with neurons, cardiac tissue, also vascular smooth muscle cells. The ATP/ADP ratio regulates them physiologically via nucleotide binding sites on the KATP channels. This allows the plasma layer to depolarize, subsequent in the prologue of voltage-subordinate calcium channels and the input of calcium particles. Calcium particles bind to calmodulin, causing insulin exocytosis to occur like that observed following glucose stimulation [65,66].
Sulfonylureas have excellent lengthy safety and effectiveness, are inexpensive, and can reduce HbA1c levels by up to 7–16 mmol/mol when taken with metformin [67]. The University Group Diabetes Program (UGDP) study suggested that Sus therapy may increase the risk of cardiovascular mortality in patients with type 2 diabetes. This investigation found that SU tolbutamide was linked to an increase in CV mortality [68]. Moreover, some experimental data suggests that SUs may raise the incidence of some cancers, including thyroid, esophageal, pancreatic, colorectal, and hepatic cancer. Possible “Downsides” of sulfonylurea use include Hypoglycemia, weight gain, and perhaps a reduction in myocardial ischemic preconditioning [69,70].
Meglitinides
Meglitinides are drugs against diabetes having an hour-long half-life that are crucial in preventing hypo- and anticipatory hyperglycemia. The two brand name medications most frequently used in this group of drugs are repaglinide and nateglinide. Repaglinide was the first meglitinide variant approved for use in T2DM patients [71]. Meglitinide is a short-acting insulin secretagogue that binds to the sulfonylurea receptor in pancreatic cells, like sulfonylureas but with weaker binding. It increases insulin secretion by inhibiting KATP channels in cells. Meglitinide responsiveness is linked to various genetic polymorphisms, including SLCO1B1, which aids in the hepatic absorption of the medication repaglinide [72].
Repaglinide is an oral medication used for type 2 diabetes, with doses ranging from 0.5 to 4 mg per meal. Meglitinides can cause minor weight gain and hypoglycemia, and individuals with mild renal and hepatic impairment should use them with caution. Repaglinide and nateglinide absorption via liver with repaglinide causing more weight gain and 10% of it eliminated by the kidney. Meglitinide therapy is associated with a 0.5 to 1.5 percent decrease in HbA1c, while repaglinide is better than nateglinide at lowering HbA1c levels [73].
Thiazolidinediones
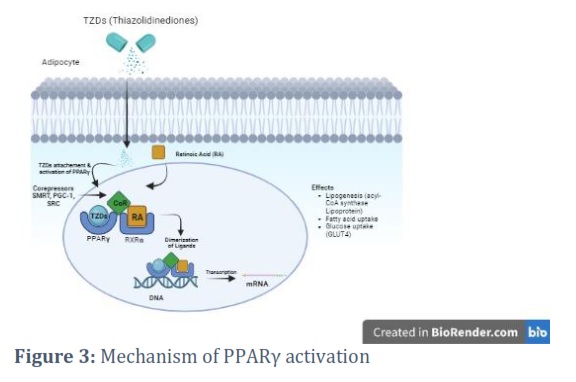
Thiazolidinediones (TZDs) are medications used for diabetes that improve insulin sensitivity in fat and muscle tissue. They help control sugar level and reduce the risk of cardio-vascular issues [74]. TZDs activate PPAR-γ, which regulates fatty acid storage and metabolism. They reduce inflammatory cytokines and increase adiponectin levels in adipose tissue, leading to sustained pancreatic beta cell function and reduced insulin resistance [75]. However, the use of TZDs has decreased because of its antagonistic properties over the last decade of fluid retention and edema caused by PPARγ activation on the nephron. TZDs have a high bioavailability and can be used in combination with metformin and sulfonylureas but are prohibited from being used with insulin due to the increased risk of weight gain. Pioglitazone is approved for use with insulin but not alone [76].
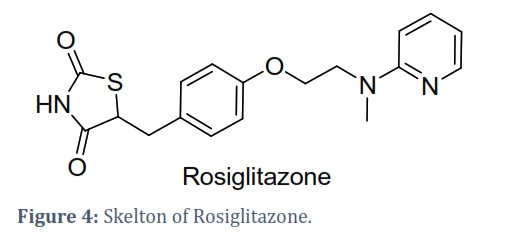
The TZDs rosiglitazone and pioglitazone have been effective in preventing and advancing albuminuria and renal fibrosis in type 2 diabetic animals. TZD therapy may retain beta cell activity, and they exhibit both PPAR-γ dependent and independent actions. Pioglitazone has been linked to bladder cancer, and both rosiglitazone and pioglitazone have been related with cardio-vascular consequence and are prohibited in many regions. However, metformin and rosiglitazone together can reduce cardio-vascular risk factors in people with T2DM or insulin resistance [77,78].
Alpha-Glucosidase Inhibitors
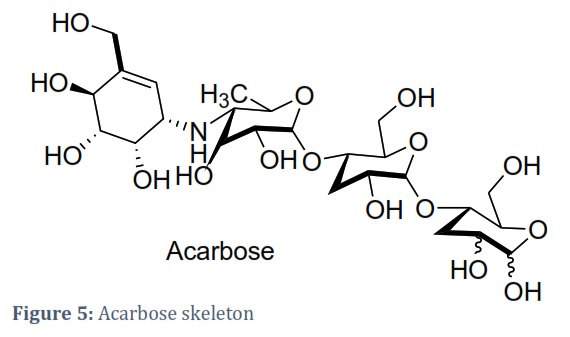
Alpha-Glucosidase (AG) inhibitors are a type of medication for diabetes that work by slowing the breakdown and absorption of carbohydrates in the small intestine. This is achieved by inhibiting the activity of the enzyme alpha-glucosidase, which breaks down complex sugars into simple sugars that can be absorbed by the body [79]. Three AGIs, including Acarbose, Miglitol, and Voglibose, are currently used in the management of diabetes. These drugs have been revealed to decrease post-prandial plasma glucose level, enhance cholesterol concentrations, blood pressure, and other cardiovascular risk factors [80]. AGIs work by blocking brush border enzymes sucrase–isomaltase and maltase-glucoamylase, which are involved in carbohydrate digestion [81]. Voglibose is commonly used to treat T2DM. AGIs have a lower risk of causing potentially fatal side effects compared to other diabetes drugs such as sulphonylureas and biguanides. In addition, the use of Acarbose has been found to lower the risk of developing T2DM in people with impaired glucose tolerance. AGIs offer an effective long-term therapy option for type 2 diabetes patients while lowering cardiovascular risk and enhancing insulin sensitivity [82].
The structure of Acarbose is presented in figure 5.
Incretin-Based Therapies
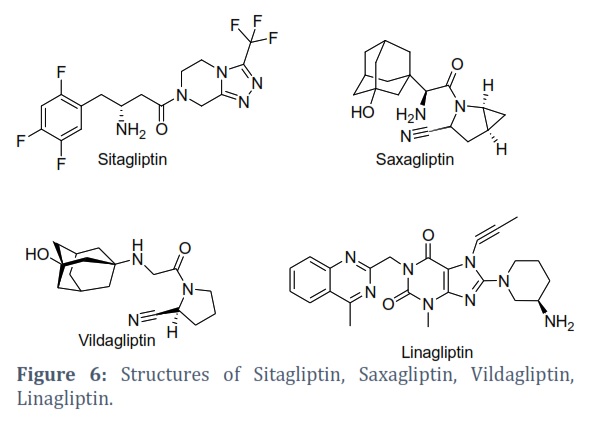
Incretin hormones are released after eating and control the release of insulin and glucagon and slowing stomach emptying and reducing the number of calories. Incretin-based medications are a recent addition to the arsenal of diabetes treatments and work by increasing beta-cell activity and insulin production while decreasing glucagon secretion. Incretin-based therapeutics are classified into two; glucagon-like peptide-1 receptor (GLP-1R) agonists and dipeptidyl peptidase-4 (DPP-4) inhibitors [83]. GLP-1 receptors are found not only in the pancreas but also in cardiovascular tissues, suggesting that GLP-1 may have cardioprotective effects. Some of the currently available drugs in this category include sitagliptin, vildagliptin, saxagliptin, linagliptin, and alogliptin. Adverse effects of incretin-based therapies include nasopharyngitis, hypersensitivity, nausea, headache, and skin reactions [84,85].
Dipeptidyl-Peptidase IV Inhibitors
Drugs that block the enzyme DPP-IV (dipeptidyl peptidase IV) are showing potential as effective treatments for diabetes. DPP-IV is responsible for breaking down GLP-1 (Glucagon-like peptide 1), a key hormone involved in regulating blood sugar levels. By inhibiting DPP-IV, GLP-1 stays active longer and can better regulate glucose levels. By inhibiting DPP-IV activity, GLP-1 and glucose-dependent insulinotropic peptide (GIP) degradation can be reduced, leading to improved incretin function and glucose homeostasis. DPP-IV cleaves the NH2-terminal amino acids of bioactive peptides, shortening GLP-1 and inactivating it. DPP IV inhibitors, such as sitagliptin, vildagliptin, saxagliptin, alogliptin, and linagliptin, improve metabolic control in type 2 diabetes, alone or in combination with other drugs [58]. Clinical studies have shown that these drugs are rapidly absorbed with high oral bioavailability and are well-tolerated with minor adverse effects [86].
Bromocriptine
Bromocriptine mesylate is an FDA-approved drug for the treatment of T2DM. The drug has been revealed a prominently lessen complete blood glucose, plasma-insulin/growth hormone concentrations during a 50 g oral glucose tolerance test in acromegaly patients when administered orally in doses of 5 mg every 6 hours for a mean of 12 months [87]. The drug acts as a postsynaptic dopamine receptor agonist and serotonin modulator and is used to treat Parkinson’s disease, hyperprolactinemia, and acromegaly [88]. It is hypothesized that bromocriptine reduces post-prandial blood glucose and hepatic glucose production by increasing low hypothalamic dopamine levels and impeding high sympathetic activity in the central nervous system by limiting serotonin turnover [89]. Daily oral doses of bromocriptine were administered to obese menopausal females, and their body fat storage was measured. In animal models, bromocriptine has been found to reset circadian rhythms and decrease body fat levels. However, an overdose of bromocriptine can lead to various symptoms, including nausea, constipation, dizziness, severe hypotension, disorientation, delusions, lethargy, and hallucinations, among others. Therefore, it is essential to monitor fluid intake and excretion closely [90].
Conclusion
We have highlighted the important classes of anti-diabetic agents and their role as oral hypoglycemic medications in the treatment of diabetes mellitus T2. Untreated diabetes can cause various problems, so it is essential to address it quickly with the right medication. Untreated diabetes can lead to complications, including diabetic retinopathy, nephropathy, and neuropathy. Other cardiovascular risk factors must also be addressed in type 2 diabetic patients. Diabetes is defined as a major chronic health disease that needs frequent self-management and an interdisciplinary team approach comprising healthcare experts, dietitians, patients understanding, and their caregivers. Diabetic patients must develop a lifestyle that allows them to control obesity and depression. Treatment choices may be personalized, or advice established on the affected risk factors, current HbA1C level, and drug efficacy, ease of use, financial situation/insurance/costs, and risk of side effects such as hypoglycemia and weight gain. The efficacy of medication must be monitored and evaluated as early as possible using diagnostic blood tests (HbA1C) and one-on-one counseling for the progression of diabetes problems such as retinopathy, nephropathy, neuropathy. Individuals with diabetes mellitus T2, an endocrine abnormality, can be managed via lifestyle modifications, careful nutrition management, and weight control. Overall, evidence from pharmacogenomics-based trials may aid in presenting a better image of any involved molecular pathways on the way to selecting pharmaco-economically feasible and applicable treatment methods for the complex multifactorial illness that is diabetes.
Author Contributions
AH, AL, MA, and MR wrote the manuscript. MA, ZR planned the proposal of the study. MR and NJ critically reviewed the manuscript. All authors contributed to the writing and editing of the manuscript. All authors have read and approved the final manuscript.
![]()
The authors declare that there is no conflict of interest.![]()
References
- Wen J, Lin T, Cai Y, Chen Q, Chen Y, et al. Baduanjin exercise for type 2 diabetes mellitus: a systematic review and meta-analysis of randomized controlled trials. Evidence-Based Complementary and Alternative Medicine, (2017); 2017.
- Raj RRR, Sahay SSS, Tripathi JTJ. Medications of diabetes mellitus and antidiabetic medicinal plants: a review. International Journal of Indigenous Herbs and Drugs, (2016); 19-28.
- Ohiagu FO, Chikezie PC, Chikezie CM. Pathophysiology of diabetes mellitus complications: Metabolic events and control. Biomed Res Ther, (2021); 8(3): 4243-4257.
- Chiefari E, Arcidiacono B, Foti D, Brunetti A. Gestational diabetes mellitus: an updated overview. Journal of endocrinological investigation, (2017); 40899-909.
- Forbes JM, Cooper ME. Mechanisms of diabetic complications. Physiological reviews, (2013); 93(1): 137-188.
- AMS DP, Mori Y, De Silva S. Self-Care among Adolescents with Type 1 Diabetes Mellitus and Nursing Care in Sri Lanka: Review of Literature. 北関東医学, (2016); 66(1): 15-22.
- Abbood M, Al-Rawi KF. Purification and characterization of Alkaline phosphatase from patients women breast cancer.
- Charan Kumar C, Murthy S. A review on management of blood glucose in type 2 diabetes mellitus. Int J Plant Sciences, (2016); 6114-120.
- Qaseem A, Barry MJ, Humphrey LL, Forciea MA, Physicians* CGCotACo. Oral pharmacologic treatment of type 2 diabetes mellitus: a clinical practice guideline update from the American College of Physicians. Annals of internal medicine, (2017); 166(4): 279-290.
- Balaji R, Duraisamy R, Kumar M. Complications of diabetes mellitus: A review. Drug Invention Today, (2019); 12(1).
- Zhuang Q-S, Shen L, Ji H-F. Quantitative assessment of the bidirectional relationships between diabetes and depression. Oncotarget, (2017); 8(14): 23389.
- Sortsoe C, Green A, Jensen PB, Emneus M. Societal costs of diabetes mellitus in Denmark. Diabetic Medicine, (2016); 33(7): 877-885.
- Tracey ML, Gilmartin M, O’Neill K, Fitzgerald AP, McHugh SM, et al. Epidemiology of diabetes and complications among adults in the Republic of Ireland 1998-2015: a systematic review and meta-analysis. BMC public health, (2015); 16(1): 1-13.
- Chen R, Ovbiagele B, Feng W. Diabetes and stroke: epidemiology, pathophysiology, pharmaceuticals and outcomes. The American journal of the medical sciences, (2016); 351(4): 380-386.
- Gonzalez JS, Esbitt SA, Schneider HE, Osborne PJ, Kupperman EG. Psychological issues in adults with type 2 diabetes. Psychological co-morbidities of physical illness: A behavioral medicine perspective, (2011); 73-121.
- Emdin CA, Rahimi K, Neal B, Callender T, Perkovic V, et al. Blood pressure lowering in type 2 diabetes: a systematic review and meta-analysis. Jama, (2015); 313(6): 603-615.
- Tao Z, Shi A, Zhao J. Epidemiological perspectives of diabetes. Cell biochemistry and biophysics, (2015); 73181-185.
- Thent ZC, Das S, Henry LJ. Role of exercise in the management of diabetes mellitus: the global scenario. PloS one, (2013); 8(11): e80436.
- Feingold KR, Anawalt B, Boyce A, Chrousos G, Dungan K, et al. Oral and injectable (non-insulin) pharmacological agents for type 2 diabetes. Endotext South Dartmouth (MA), (2020).
- Adisakwattana S. Cinnamic acid and its derivatives: mechanisms for prevention and management of diabetes and its complications. Nutrients, (2017); 9(2): 163.
- Crews KR, Hicks JK, Pui CH, Relling MV, Evans WE. Pharmacogenomics and individualized medicine: translating science into practice. Clinical Pharmacology & Therapeutics, (2012); 92(4): 467-475.
- Bansal R, Agarwal P. Prevalence of Diabetes and Hypertension among Adults 20 Yrs and above in Urban Slums of Delhi. Call for Editorial Board Members, 65.
- Ismail-Beigi F, Craven T, Banerji MA, Basile J, Calles J, et al. Effect of intensive treatment of hyperglycaemia on microvascular outcomes in type 2 diabetes: an analysis of the ACCORD randomised trial. The Lancet, (2010); 376(9739): 419-430.
- Phan DH, Do VV, Khuong LQ, Nguyen HT, Minh HV. Prevalence of diabetes and prediabetes among children aged 11-14 years old in Vietnam. Journal of Diabetes Research, (2020); 2020.
- O'neill D, Gostelow R, Orme C, Church D, Niessen S, et al. Epidemiology of diabetes mellitus among 193,435 cats attending primary‐care veterinary practices in England. Journal of Veterinary Internal Medicine, (2016); 30(4): 964-972.
- Deshpande AD, Harris-Hayes M, Schootman M. Epidemiology of diabetes and diabetes-related complications. Physical therapy, (2008); 88(11): 1254-1264.
- Craig ME, Hattersley A, Donaghue KC. Definition, epidemiology and classification of diabetes in children and adolescents. Pediatr diabetes, (2009); 10(Suppl 12): 3-12.
- Ma W-T, Chang C, Gershwin ME, Lian Z-X. Development of autoantibodies precedes clinical manifestations of autoimmune diseases: A comprehensive review. Journal of autoimmunity, (2017); 8395-112.
- Patterson C, Guariguata L, Dahlquist G, Soltész G, Ogle G, et al. Diabetes in the young–a global view and worldwide estimates of numbers of children with type 1 diabetes. Diabetes research and clinical practice, (2014); 103(2): 161-175.
- Zimmet PZ, Alberti KGM. Epidemiology of diabetes—status of a pandemic and issues around metabolic surgery. Diabetes care, (2016); 39(6): 878-883.
- Basit A, Fawwad A, Qureshi H, Shera A. Prevalence of diabetes, pre-diabetes and associated risk factors: second National Diabetes Survey of Pakistan (NDSP), 2016–2017. BMJ open, (2018); 8(8): e020961.
- Morran MP, Vonberg A, Khadra A, Pietropaolo M. Immunogenetics of type 1 diabetes mellitus. Molecular aspects of medicine, (2015); 4242-60.
- Cruz NG, Sousa LP, Sousa MO, Pietrani NT, Fernandes AP, et al. The linkage between inflammation and Type 2 diabetes mellitus. Diabetes research and clinical practice, (2013); 99(2): 85-92.
- Kumar Arora M, Kumar Singh U. Oxidative stress: meeting multiple targets in pathogenesis of diabetic nephropathy. Current drug targets, (2014); 15(5): 531-538.
- Evans JL, Goldfine ID, Maddux BA, Grodsky GM. Are oxidative stress− activated signaling pathways mediators of insulin resistance and β-cell dysfunction? Diabetes, (2003); 52(1): 1-8.
- Juszczyk A, Jankowska K, Zawiślak B, Surdacki A, Chyrchel B. Depressed cardiac mechanical energetic efficiency: a contributor to cardiovascular risk in common metabolic diseases—from mechanisms to clinical applications. Journal of clinical medicine, (2020); 9(9): 2681.
- Hameed I, Masoodi SR, Mir SA, Nabi M, Ghazanfar K, et al. Type 2 diabetes mellitus: from a metabolic disorder to an inflammatory condition. World journal of diabetes, (2015); 6(4): 598.
- Rains JL, Jain SK. Oxidative stress, insulin signaling, and diabetes. Free radical biology and medicine, (2011); 50(5): 567-575.
- Niki E. Lipid peroxidation products as oxidative stress biomarkers. Biofactors, (2008); 34(2): 171-180.
- Shabalala SC, Johnson R, Basson AK, Ziqubu K, Hlengwa N, et al. Detrimental Effects of Lipid Peroxidation in Type 2 Diabetes: Exploring the Neutralizing Influence of Antioxidants. Antioxidants, (2022); 11(10): 2071.
- Mazur-Bialy A, Kozlowska K, Pochec E, Bilski J, Brzozowski T. Myokine irisin-induced protection against oxidative stress in vitro. Involvement of heme oxygenase-1 and antioxidazing enzymes superoxide dismutase-2 and glutathione peroxidase. J Physiol Pharmacol, (2018); 69(1): 117-125.
- Gerber PA, Rutter GA. The role of oxidative stress and hypoxia in pancreatic beta-cell dysfunction in diabetes mellitus. Antioxidants & redox signaling, (2017); 26(10): 501-518.
- Kochikuzhyil BM (2009) Evaluation of Dyslipidemic Effect Of Dietary Vegetable Oils Under Stress And Non-Stress Conditions In Normal And Diabetic Rats: Rajiv Gandhi University of Health Sciences (India).
- Agrawal NK, Kant S. Targeting inflammation in diabetes: Newer therapeutic options. World journal of diabetes, (2014); 5(5): 697.
- Alipourfard I, Datukishvili N, Mikeladze D. TNF-α downregulation modifies insulin receptor substrate 1 (IRS-1) in metabolic signaling of diabetic insulin-resistant hepatocytes. Mediators of inflammation, (2019); 2019.
- Vaxillaire M, Froguel P. Best Practice & Research Clinical Endocrinology & Metabolism. Best Practice & Research Clinical Endocrinology & Metabolism, (2012); 26171-187.
- Lavin DP, White MF, Brazil DP. IRS proteins and diabetic complications. Diabetologia, (2016); 59(11): 2280-2291.
- Arikoglu H, Hepdogru MA, Kaya DE, Asik A, Ipekci SH, et al. IRS1 gene polymorphisms Gly972Arg and Ala513Pro are not associated with insulin resistance and type 2 diabetes risk in non-obese Turkish population. Meta gene, (2014); 2579-585.
- Sanchez-Rangel E, Inzucchi SE. Metformin: clinical use in type 2 diabetes. Diabetologia, (2017); 601586-1593.
- Herman R, Kravos NA, Jensterle M, Janež A, Dolžan V. Metformin and insulin resistance: a review of the underlying mechanisms behind changes in GLUT4-mediated glucose transport. International Journal of Molecular Sciences, (2022); 23(3): 1264.
- Rena G, Hardie DG, Pearson ER. The mechanisms of action of metformin. Diabetologia, (2017); 60(9): 1577-1585.
- Kinaan M, Ding H, Triggle CR. Metformin: an old drug for the treatment of diabetes but a new drug for the protection of the endothelium. Medical principles and practice, (2015); 24(5): 401-415.
- Freeland B, Farber MS. Type 2 diabetes drugs: a review. Home healthcare now, (2015); 33(6): 304-310.
- de Souza GS, Mantovani DB, Mossel P, Haarman BC, da Silva AMM, et al. Oral administration of PET tracers: Current status. Journal of Controlled Release, (2023); 357591-605.
- Osadebe PO, Odoh EU, Uzor PF. Oral anti-diabetic agents-review and updates. Management, (2015); 21.
- Kupsal K, Mudigonda S, Sai N, Neelala K, Hanumanth S. Metformin combinatorial therapy for type 2 diabetes mellitus. J Metab Syndr, (2016); 5(3): 1000210.
- Gautam D, Gautam D. A Short Review On Anti-Diabetic Agent. PharmaTutor, (2014); 2(10): 89-105.
- Popovic-Djordjevic JB, Jevtic II, Stanojkovic TP. Antidiabetics: structural diversity of molecules with a common aim. Current Medicinal Chemistry, (2018); 25(18): 2140-2165.
- Hemmingsen B, Schroll JB, Wetterslev J, Gluud C, Vaag A, et al. Sulfonylurea versus metformin monotherapy in patients with type 2 diabetes: a Cochrane systematic review and meta-analysis of randomized clinical trials and trial sequential analysis. Canadian Medical Association Open Access Journal, (2014); 2(3): E162-E175.
- White Jr JR. A brief history of the development of diabetes medications. Diabetes spectrum: a publication of the American Diabetes Association, (2014); 27(2): 82.
- CHAUHAN M, VARMA AK. Indian Journal of Novel Drug Delivery. Indian Journal of Novel Drug Delivery, (2022); 14(1): 8-15.
- Hirst J, Farmer A, Dyar A, Lung T, Stevens R. Estimating the effect of sulfonylurea on HbA 1c in diabetes: a systematic review and meta-analysis. Diabetologia, (2013); 56973-984.
- Chaudhury A, Duvoor C, Reddy Dendi VS, Kraleti S, Chada A, et al. Clinical review of antidiabetic drugs: implications for type 2 diabetes mellitus management. Frontiers in endocrinology, (2017); 86.
- Deacon C, Lebovitz HE. Comparative review of dipeptidyl peptidase‐4 inhibitors and sulphonylureas. Diabetes, Obesity and Metabolism, (2016); 18(4): 333-347.
- Yang M, Dart C, Kamishima T, Quayle JM. Hypoxia and metabolic inhibitors alter the intracellular ATP: ADP ratio and membrane potential in human coronary artery smooth muscle cells. PeerJ, (2020); 8e10344.
- So WY, Liu WN, Teo AKK, Rutter GA, Han W. Paired box 6 programs essential exocytotic genes in the regulation of glucose-stimulated insulin secretion and glucose homeostasis. Science Translational Medicine, (2021); 13(600): eabb1038.
- Gunton JE, Cheung NW, Davis TME, Zoungas S, Colagiuri S. A new blood glucose management algorithm for type 2 diabetes: a position statement of the Australian Diabetes Society. Medical journal of Australia, (2014); 201(11): 650-653.
- Forst T, Hanefeld M, Jacob S, Moeser G, Schwenk G, et al. Association of sulphonylurea treatment with all-cause and cardiovascular mortality: a systematic review and meta-analysis of observational studies. Diabetes and Vascular Disease Research, (2013); 10(4): 302-314.
- Chen Y, Du L, Li L, Ma J, Geng X, et al. Cancer risk of sulfonylureas in patients with type 2 diabetes mellitus: A systematic review. Journal of Diabetes, (2017); 9(5): 482-494.
- Farahani P, Khan S, Oatway M, Dziarmaga A. Exploring the distribution of prescription for sulfonylureas in patients with type 2 diabetes according to cardiovascular risk factors within a Canadian primary care setting. Journal of Population Therapeutics and Clinical Pharmacology, (2015); 22(3).
- Wu P-C, Wu V-C, Lin C-J, Pan C-F, Chen C-Y, et al. Meglitinides increase the risk of hypoglycemia in diabetic patients with advanced chronic kidney disease: a nationwide, population-based study. Oncotarget, (2017); 8(44): 78086.
- Guardado-Mendoza R, Prioletta A, Jiménez-Ceja LM, Sosale A, Folli F. State of the art paper The role of nateglinide and repaglinide, derivatives of meglitinide, in the treatment of type 2 diabetes mellitus. Archives of medical science, (2013); 9(5): 936-943.
- Brunetti L, Kalabalik J. Management of type-2 diabetes mellitus in adults: focus on individualizing non-insulin therapies. Pharmacy and therapeutics, (2012); 37(12): 687.
- Rizos CV, Elisaf M, Mikhailidis DP, Liberopoulos EN. How safe is the use of thiazolidinediones in clinical practice? Expert opinion on drug safety, (2009); 8(1): 15-32.
- Rathwa N, Patel R, Palit SP, Parmar N, Rana S, et al. β-cell replenishment: Possible curative approaches for diabetes mellitus. Nutrition, Metabolism and Cardiovascular Diseases, (2020); 30(11): 1870-1881.
- Della-Morte D, Palmirotta R, Rehni AK, Pastore D, Capuani B, et al. Pharmacogenomics and pharmacogenetics of thiazolidinediones: role in diabetes and cardiovascular risk factors. Pharmacogenomics, (2014); 15(16): 2063-2082.
- Goltsman I, Khoury EE, Winaver J, Abassi Z. Does Thiazolidinedione therapy exacerbate fluid retention in congestive heart failure? Pharmacology & Therapeutics, (2016); 16875-97.
- Lu P, Zhao Z. Advances on PPARγ research in the emerging era of precision medicine. Current drug targets, (2018); 19(6): 663-673.
- Kalra S. Alpha glucosidase inhibitors. JPMA The Journal of the Pakistan Medical Association, (2014); 64(4): 474-476.
- Hedrington MS, Davis SN. Considerations when using alpha-glucosidase inhibitors in the treatment of type 2 diabetes. Expert opinion on pharmacotherapy, (2019); 20(18): 2229-2235.
- Kashtoh H, Baek K-H. Recent Updates on Phytoconstituent Alpha-Glucosidase Inhibitors: An Approach towards the Treatment of Type Two Diabetes. Plants, (2022); 11(20): 2722.
- Suzuki K, Katsura D, Sagara M, Aoki C, Nishida M, et al. Postprandial reactive hypoglycemia treated with a low-dose alpha-glucosidase Inhibitor: Voglibose may suppress oxidative stress and prevent endothelial dysfunction. Internal Medicine, (2016); 55(8): 949-953.
- Peters A. Incretin-based therapies: review of current clinical trial data. The American journal of medicine, (2010); 123(3): S28-S37.
- Garber AJ. Incretin-based therapies in the management of type 2 diabetes: rationale and reality in a managed care setting. American Journal of Managed Care, (2010); 16(7): S187.
- Ceriello A, Sportiello L, Rafaniello C, Rossi F. DPP-4 inhibitors: pharmacological differences and their clinical implications. Expert opinion on drug safety, (2014); 13(sup1): 57-68.
- Singh A-K, Yadav D, Sharma N, Jin J-O. Dipeptidyl Peptidase (DPP)-IV inhibitors with antioxidant potential isolated from natural sources: A novel approach for the management of diabetes. Pharmaceuticals, (2021); 14(6): 586.
- Naz F, Malik A, Riaz M, Mahmood Q, Mehmood MH, et al. Bromocriptine therapy: Review of mechanism of action, safety and tolerability. Clinical and Experimental Pharmacology and Physiology, (2022); 49(8): 903-922.
- Bandala C, Cárdenas-Rodríguez N, Mendoza-Torreblanca JG, Contreras-García IJ, Martínez-López V, et al. Therapeutic Potential of Dopamine and Related Drugs as Anti-Inflammatories and Antioxidants in Neuronal and Non-Neuronal Pathologies. Pharmaceutics, (2023); 15(2): 693.
- Oshige T, Nakamura Y, Sasaki Y, Kawano S, Ohki T, et al. Bromocriptine as a potential glucose-lowering agent for the treatment of prolactinoma with type 2 diabetes. Internal Medicine, (2019); 58(21): 3125-3128.
- Keche Y. Bromocriptine mesylate: Food and Drug Administration approved new approach in therapy of non-insulin dependant diabetes mellitus with poor glycemic control. Journal of Pharmacy And Bioallied Sciences, (2010); 2(2): 148.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0