

Full Length Research Article
Morphological Identification and Resistance Profile of Antibiotic and Heavy Metals-Resistant Bacteria in Hospital Sewage of Peshawar
Muhammad Ijaz1, Gulzar Ahmad1, Farida Anjum2, Usman Zeb3, Noor Muhammad4, Irfan Khan5, Sidra Usman1, Abrar Hussain1, Shumaila Ubaid6, Abdul Haseeb Rahim1, Umbarin Latif2, Humaira Gul2, Rahim Shah7, Hafsa Shah1, Faryal Azam1, Zia Ur Rahman8, Muhammad Ayaz9, Ahmad Usman Zafar10, Faraz Ahmad Khan1, Hafiza Wajeeha Zahid1, Sulaiman Faisal1*
Adv. life sci., vol. 10, no. 3, pp. 452-456, September 2023
*– Corresponding Author: Sulaiman Faisal (sulaiman@cecos.edu.pk)
Authors' Affiliations
2. Agriculture Research Institute (ARI) Tarnab Peshawar – Pakistan
3. Institute of Biotechnology and Genetic Engineering (IBGE) ,University of Agriculture Peshawar – Pakistan
4. Department of Microbiology Kohat University KPK – Pakistan
5. Khyber Medical University Peshawar – Pakistan
6. PEF Post Graduate College Peshawar – Pakistan
7. National Institute of Health Islamabad – Pakistan
8. National Centre of Excellence in Molecular Biology, University of the Punjab – Pakistan
9. Center of Biotechnology and Microbiology, University of Peshawar – Pakistan
10. Department of Biotechnology, Qarshi University, Canal Road, Lahore – Pakistan
[Date Received: 11/05/2023; Date Revised: 23/06/2023; Date Published Online: 30/09/2023; Date Updated: 06/09/2025]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Increased resistance of microorganisms to commonly prescribed antibiotics has emerged as a significant hurdle in contemporary medical practice. The World Health Organization (WHO) has declared antibiotic resistance as a " major threat to public health.". In the present study, bacterial isolates were selected based on high antibiotic and heavy metal tolerance from a water sample taken from hospital sewage.
Methods: Antibiotic-resistant bacteria were isolated through the disk diffusion method. Gram staining was done for morphological identification. For molecular identification, the 16s rDNA PCR amplification was done with universal primers.
Results: The strain BC1 was resistant to ampicillin (10 µg/ml) and cefixime (5 µg/ml), while it was susceptible to kanamycin (30 µg/ml) and azithromycin (15 µg/ml), and showed an intermediate response to amoxicillin (30 µg/ml). The strain BC2 was resistant to ampicillin (10 µg/ml), cefixime (5 µg/ml), and kanamycin (30 µg/ml), while it was susceptible to amoxicillin (30 µg/ml) and showed an intermediate response to azithromycin (15 µg/ml). Both strains were also found resistant to heavy metals.
Conclusion: The recent investigation on bacterial strains from hospital effluent identified interesting candidates for understanding antimicrobial resistance (AMR) and for developing novel bioactive molecules to address the challenge of antibiotic resistance. The isolated strains may serve as a potential source of novel resistance genes; however, comprehensive molecular analyses are required for future advanced studies.
Keywords: Multidrug resistance; Bacteria; Heavy metal; Hospital sewage; Amoxicillin; Archaea; Azithromycin
Introduction![]()
Microorganisms are present everywhere in the ecosystem. Microorganisms are divided into different classes, i.e., bacteria, archaea and fungi. Bacteria are present in the human body and play vital roles in our body, in digestion and in protecting our skin among other important benefits [1]. There is an approximate estimation that the Earth harbors around one trillion distinct microbial species, the majority of which remain unfamiliar to our understanding [2-4]. While certain microbial species play a vital role in our survival, a minority of bacteria can be responsible for causing diseases in humans, animals, and plants. These bacteria are known as pathogenic bacteria and have some serious effects on human health [5,6]. Antibiotics hold significant value as medicinal treatments for bacterial infections and serve as essential elements within healthcare systems [7]. Over the past 80 years, the widespread utilization of antibiotics on a global scale has given rise to progressively alarming issues due to the emergence of bacteria that are resistant to these drugs [8,9]. These challenges result in hundreds of thousands of annual fatalities and are anticipated to escalate significantly in the future [10,11]. The use of antibiotics would introduce complications into various healthcare procedures, including surgery, cancer treatment, and patient care [12]. Antibiotic resistance develops when either antibiotics are overprescribed, or a proper/sufficient dose is not prescribed which leads to resistance towards antibiotics. Recognizing antibiotic resistance as a significant peril to human health, the World Health Organization (WHO) has acknowledged its significance [13]. The emergence of antibiotic-resistant bacteria is influenced by the environment, which holds a crucial role in this process. The external surroundings serve as a reservoir for resistance genes that can be transmitted to human pathogens. Moreover, the environment acts as a significant pathway for the transfer of antibiotic resistance genes and bacteria [12,14]. Hospitals, including their sewage systems, are significant pathways through which genes responsible for antibiotic resistance are released into the environment [15]. There is a suggestion that hospitals and their sewage systems act as hotspots for the emergence of antibiotic resistance due to their elevated levels of antibiotics and the presence of both human-associated and environmental bacteria. Furthermore, complicating the situation further, there is evidence indicating that other antimicrobial substances like antiseptics and metals can contribute to the development of antibiotic resistance [12,16]. The identification of the pure culture is done through morphological identification by performing Gram staining and observing the colony characteristics of the pure colony [4]. The 16s rDNA sequence is used for the molecular identification of pure strains. By separating the genomic DNA, bacteria can be identified molecularly. Polymerase chain reaction (PCR) generates copies of DNA sequence and then bacterial identification based on 16S ribosomal DNA (rDNA). Bacterial phylogeny and taxonomy are examined using 16S rRNA gene sequences . It is present in almost all, bacteria. We are able to study morphology, metabolism, physiology and can identify bacteria through 16S rDNA molecular techniques. The antibiotic resistance is due to the presence of genes on plasmid or chromosomal DNA in bacteria. Plasmid has different functions. They may contain different genes which are important for the survival of an organism. The plasmid is due to killing the other organism or defending the host cell. Some plasmids help in replication. The plasmid is small and contains few genes with specific functions [17].
The main objective of that study was to isolate antibiotic-resistant bacterial strains from the govt hospitals effluent of Peshawar area.
Methods![]()
Study area
The present study on antibiotic-resistant bacteria from hospital sewage was conducted in the Microbiology Laboratory, Department of Biotechnology, Institute of Integrative Biosciences, CECOS University, Peshawar, from September 2020 to March 2021.
Sample collection
The sample was collected from hospital effluent in the Peshawar area, KPK. The sample was collected in 50 ml sterile falcon tubes and then brought into the lab for further analysis. During sample collection some important parameters were recorded i.e., pH 7, temperature 30°C and GPS coordinates were Lt 33.9966° L 71.4860°. The samples were brought to the lab for further analysis.
Isolation of the bacterial strains
For the isolation of the bacterial strains, Luria Bertani (LB) agar media was prepared. 100 µl of water sample was inoculated on 20 ml LB/Agar plate via spread plate method. The plate was incubated at 37°C, overnight. Two colonies were selected for further analysis based on shape and color.
Screening of the isolates in the presence of antibiotics
Antibiotic tolerance of the selected isolates, BC1 and BC2 was checked through the Kirby-Bauer disc diffusion method. 20ml LB/Agar plates were prepared. 100 µl inoculum from the fresh overnight cultures of BC1 and BC2 was used to make a bacterial lawn on the agar plates through a glass spreader. Antibiotic discs; ampicillin (10μg/ml), azithromycin (15μg/ml), cefixime (5μg/ml), kanamycin (30μg/ml) and amoxicillin (30μg/ml) were then placed on the respective agar plates. The plates were incubated at 37°C, overnight. Zone sizes were measured after 24 hours.
Heavy metal tolerance of the strains
Stock solutions of the metals; zinc, cadmium, cobalt and chromium were prepared. The working concentrations against which the two isolates' tolerance was checked were (5 mM, 7 mM, 9 mM, 10 mM 11 mM, 13 mM,14mM, 15mM, 18mM, 20 mM). 100ul inoculum from the overnight cultures of both the isolates was spread on 20ml LB/Agar plates supplemented with metal salts. The plates were incubated at 37°C, overnight.
Gram Staining and Genomic DNA extraction
To differentiate and classify the bacterial isolates, Gram staining was performed for morphological identification. A bacterial smear was prepared on a slide from the fresh overnight culture. The prepared slides were observed under the microscope. For molecular characterization, Genomic and plasmid DNA was extracted through CTAB and manual extraction methods [18].
16S rDNA PCR amplification and Gel electrophoresis
For DNA amplification, PCR with 16S universal primers was performed. The universal primers used were 27F and 1392R. A PCR master mix was prepared for the DNA sample and the positive and negative controls. DNA samples were observed through gel electrophoresis. 1% agarose gel was made in TAE buffer. 0.5g of agarose was added to 50 ml of 1X TAE buffer and heated until the agarose was completely dissolved. DNA samples and the control DNA samples were loaded. 1ul of 6X loading dye was mixed with 5ul of DNA samples. The gel was run at 80V for 60 minutes. DNA bands were observed in the gel documentation system.
Results![]()
Isolation of the bacterial strains
Initially, a total of 50 colonies were observed on LB/Agar plates after the inoculation of a water sample. Among these colonies, two colonies were selected and purified randomly for antibiotic and heavy metal tolerance analysis. Optimum growth was examined in LB agar media, and LB. The favourable temperature is 37°C and pH is 7.5 and the tolerance of the strains towards heavy metals is Cd>Zn>Cr = Co, shown in Figure 1a-b.
Screening of the isolates in the presence of antibiotics
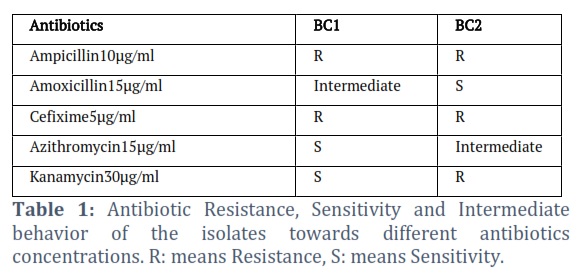
Through the disc diffusion method, the antibiotic resistance of the isolates BC1 and BC2 was checked. Based on size of the zone of inhibition, the strain BC1 was found resistant to ampicillin 10μg/ml and cefixime 5μg/ml. It was sensitive to kanamycin 30μg/ml and azithromycin15μg/ml and intermediate to amoxicillin15μg/ml. The strain BC2 was resistant to ampicillin 10μg/ml, cefixime 5μg/ml and Kanamycin 30μg/ml. It was found sensitive to amoxicillin 15μg/ml and intermediate to azithromycin15μg/ml. Results are shown in Figure 2a-c. the sizes of zone of inhibition are shown in Table 1.
Heavy metal tolerance of the isolates
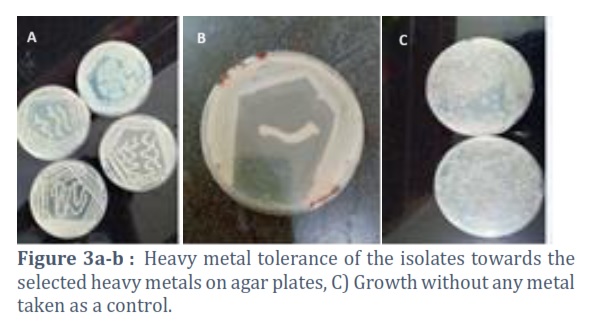
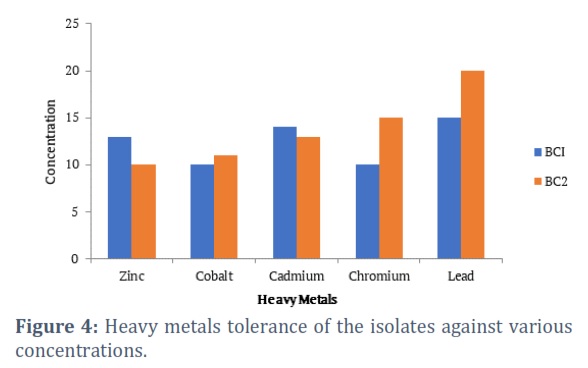
The strains were checked against varying concentrations of heavy metals. The strain BC1 was resistant to 10, 15, 14, 13, and 10 mM of chromium, lead, cadmium, zinc and cobalt respectively. While the strain BC2 was resistant to 15, 20, 13, 10 and 11 mM of chromium, lead, cadmium, zinc and cobalt respectively. The order of tolerance to the heavy metals of the strains is as follows: Pb > Cd > Zn > Cr > Co for BC1 and Pb > Cr > Cd > Co > Zn for BC2. Different growth is shown in Figures 3a-c and 4.
Morphological and Molecular analysis
Genomic and Plasmid DNA extraction
Gram staining results of both isolates are shown in Figure 5a-b and Table 2. The genomic DNA of the isolates was successfully extracted through the CTAB method and run on 1% agarose gel at 80V and insert the gel picture of the genomic DNA of both isolates. Plasmid DNA was extracted and the DNA was run on 1% agarose gel at 80V for 60 minutes.
16S rDNA PCR
16S PCR of the isolates was done and the positive, negative control and bacterial isolates DNA bands are 1500 bp DNA band were observed after 16S PCR with universal primers 1500 base pairs apart.
Figures & Tables


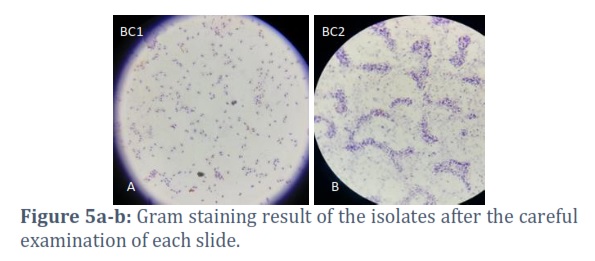
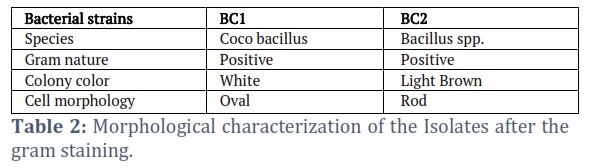
In this study, a hospital effluent water sample was collected from Khyber Teaching Hospital Peshawar. Antibiotic-resistant bacteria were isolated through the disk diffusion method on LB/ Agar plate. The bacterial isolate that showed the highest resistance was selected from the Agar plates and supplemented with different antibiotic disks. Gram staining was done for morphological identification, and according to Bergey’s Manual, the morphological characterization identified BC1 as Cocobacillus and BC2 as Bacillus spp. (Table 2). For molecular identification, the 16s rDNA PCR amplification was done with universal primers. Antibiotics play a crucial role as essential medications employed in the treatment of bacterial infections and serve as vital components within healthcare systems [12]. Antibiotics inhibit the growth of bacteria. They diffuse from the disc into the surrounding agar medium and inhibit the growth of bacteria. Different antibiotics differ in their effect on different bacteria. It is useful to check the sensitivity of different bacteria for antibiotics. People who use antibiotics frequently have bacteria that are resistant to antimicrobial drugs. Since an antibiotic’s interaction with a target molecule is very selective, even little variations in the target molecule can affect an antibiotic’s ability to bind to the target [19]. Azithromycin can occasionally change a particular target when RNA polymerase is present to carry out the transcriptional modification. Amoxicillin binds to the 50S ribosomal subunit and inhibits protein synthesis, whereas Kanamycin binds to the 30S ribosomal subunit [20]. To defend themselves, bacteria employ both inherent and evolved resistance mechanisms. Mutations, gene transfer via conjugation or transformation, transposons, integrons, and bacteriophages are all sources of acquired resistance. Bacteria use biochemical resistance strategies such as metabolic route “bypass,” target alteration, altered permeability, and antibiotic inactivation. It’s important to identify the kinds of antibiotics and mutations that bacteria are resistant to to develop effective therapies [5]. A plasmid that mediates Resistance is disseminated throughout the world by horizontal plasmid-borne migration [2]. Most resistance plasmids are mobilizable or conjugative. Both a wide and a limited host range are displayed by conjugative plasmids. A process called conjugation is used to transfer genes from donor to recipient cells that have undergone homologous recombination, integration, and excision from the host chromosome. These plasmid-encoded complexes assist the donor by binding to potential recipients, which results in the creation of secured associations, which are necessary before the translocation of DNA. Mobilizable plasmids have DNA transfer genes necessary for the structure of all or a portion of the relaxasome, but they lack the genes important for the production of the mating pore. They can use conjugative plasmids for horizontal expansion, but they are immovable in cells lacking mobile elements carrying suitable mating-pore genes [21]. The recent investigation on bacterial strains from hospital effluent found interesting candidates for understanding the evolution of environmental resistomes and developing novel active bio-molecules to combat the antibiotics problem. In hospitals, the wastewater has no proper treatment and this water directly impacts the food chain which is the main reason for the multidrug-resistant bacteria.
The risk with antibiotic resistance is that it is contagious. After administration, the bulk of antibiotics is only partially digested and discharged via patient excretion into the hospital sewage system. According to earlier findings, antibiotic-resistant bacteria from the environment could spread to humans and infect them with diseases that cannot be cured with regular antibiotics. Questions have arisen over the best way to address the issue of antibiotic resistance. In developing countries, improved sewage infrastructure and general public health initiatives can help avoid infection. This study shows the high prevalence of resistant bacteria spread in the environment. Further studies on molecular screening and genomic analysis may be conducted to identify specific genes related to antimicrobial resistance.
Acknowledgement
I would like to thank the Institute of Integrative Biosciences, Cecos University Peshawar for providing us their lab and all the research materials and Special thanks to each of my classmates whose support has helped us to complete this research.
Competing Interest
All authors of this work have declared that there is no conflict of interest
Dr.Sulaiman Faisal, and Dr. Farida Anjum supervised the project. Muhammad Ijaz, Gulzar Ahmad, Sidra Usman, Abrar Hussain, Rahim Shah, Faraz Ahmad Khan, Shumaila Ubaid, Abdul Haseeb Rahim, Irfan, Umbarin Latif, Humaira Gul, Usman Zeb, Faryal Azam, Noor Muhammad, Muhammad Ayaz, Hafsa Shah, Zia Ur Rahman, Ahmad Usman Zafar, Hafiza Wajeeha Zahid perform and analyze the experiments, all the authors have written the manuscript, reviewed the manuscript and agreed to submit it.
![]()
References
- Martiny JBH, Bohannan BJ, Brown JH, Colwell RK, Fuhrman JA, et al. Microbial biogeography: putting microorganisms on the map. Nature Reviews Microbiology (2006); 4(2): 102-112.
- Carattoli A. Plasmids and the spread of resistance. International journal of medical microbiology, (2013); 303(6-7): 298-304.
- Casadevall A, Pirofski L-a. Microbiology: ditch the term pathogen. Nature, (2014); 516(7530): 165-166.
- Coico R. Gram staining. Current protocols in microbiology, (2006); (1): A. 3C. 1-A. 3C. 2.
- Giedraitienė A, Vitkauskienė A, Naginienė R, Pavilonis A. Antibiotic resistance mechanisms of clinically important bacteria. Medicina, (2011); 47(3): 19.
- Anwar M, Ejaz M, Ijaz M, Ahmad G, Ayub H, et al. Association of IL-17A promoter region SNP-rs2275913 with urinary bladder cancer, " International Journal of Health Sciences (2023); 17(3): 33.
- Khan A, Ahmad G, Ijaz M, Ahsan K, Akhtar H, et al. Prevalence and Antibiotic Resistance of Salmonella Species Isolated from Chicken Liver in Peshawar. Journal of Clinical and Medical Research (2021); 3(3): 1-11.
- Hussain T, Usman S, Khan A, Hussain A, Aziz A, et al. Isolation and Characterization of Salt Tolerant Bacteria from Saline Areas of Khyber Pakhtunkhwa. Journal of Clinical and Medical Research (2022); 4(4): 1-8.
- Rahim A, Ahmad G, Ijaz M, Akhtar H, Ahsan K, et al. Isolation and Identification of Antibiotics Susceptible Staph aureus from Unprocessed Milk. Journal of Clinical and Medical Research (2021); 3(2): 1-11.
- Ashbolt NJ, Amézquita A, Backhaus T, Borriello P, Brandt KK, et al. Human health risk assessment (HHRA) for environmental development and transfer of antibiotic resistance. Environmental health perspectives, (2013); 121(9): 993-1001.
- Ullah S, Rahman W, Ullah F, Ahmad G, Ijaz M, et al. DBHR: a collection of databases relevant to human research. Future Science OA, (2022); 8(3): FSO780.
- Hegstad K, Langsrud S, Lunestad BT, Scheie AA, Sunde M, et al. Does the wide use of quaternary ammonium compounds enhance the selection and spread of antimicrobial resistance and thus threaten our health? Microbial drug resistance, (2010); 16(2): 91-104.
- Ullah S, Ullah A, Rahman W, Ullah F, Khan SB, et al. An innovative user-friendly platform for Covid-19 pandemic databases and resources. Computer Methods and Programs in Biomedicine Update, (2021); 1100031.
- Stallins JA, Strosberg S. Ontology, difference, and the antimicrobial resistance timeline. Futures, (2019); 102467.
- Ullah S, Ullah F, Karras DA, Rahman W, Ahmad G, et al. CRDB: A Centralized Cancer Research DataBase and an example use case mining correlation statistics of cancer and covid-19. Journal of Medical Internet Research cancer, (2022) 8(2): 35020.
- Casadevall A, Pirofski L-a. Microbiology: ditch the term pathogen. Nature News, (2014); 516(7530): 165.
- Rodriguez-Mozaz S, Chamorro S, Marti E, Huerta B, Gros M, et al. Occurrence of antibiotics and antibiotic resistance genes in hospital and urban wastewaters and their impact on the receiving river. Water research, (2015); 69234-242.
- Guertler P, Harwardt A, Eichelinger A, Muschler P, Goerlich O, et al. Development of a CTAB buffer-based automated gDNA extraction method for the surveillance of GMO in seed. European Food Research and Technology, (2013); 236(4): 599-606.
- Singer AC, Shaw H, Rhodes V, Hart A. Review of antimicrobial resistance in the environment and its relevance to environmental regulators. Frontiers in microbiology, (2016); 7, 1728 .
- Vitkauskienė A, Giedraitienė A, Dudzevičius V, Sakalauskas R. Relationship between isolation of extended spectrum beta-lactamase-producing Klebsiella pneumoniae and course of hospital-acquired pneumonia. Medicina, (2007); 43(10): 778.
- Holmes AH, Moore LS, Sundsfjord A, Steinbakk M, Regmi S, et al. Understanding the mechanisms and drivers of antimicrobial resistance. The Lancet, (2016); 387(10014): 176-187.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0