

Short Communication
Genetic Characterization of Carbapenem Resistant Acinetobacter baumannii in Tertiary care settings of Lahore, Pakistan
Saadia Ijaz1*, Farheen Ansari1, Muhammad Nawaz2, Aftab Ahmad Anjum2, Karam Rasool3
Adv. life sci., vol. 10, no. 3, pp. 479-485, September 2023
*– Corresponding Author: Saadia Ijaz (silverpinball@yahoo.com)
Authors' Affiliations
2. University of Veterinary and Animal Sciences, Lahore – Pakistan
3. Chughtai Institute of Pathology, Lahore – Pakistan
[Date Received: 11/04/2022; Date Revised: 18/08/2023; Date Published Online: 30/09/2023; Date Updated: 06/09/2025]
Editorial Note on Version of Record
24 June 2025: This article has been corrected. See https://doi.org/10.62940/als.v13i0.4220 for more information.
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Acinetobacter baumannii is major cause of ventilator associated pneumonia (VAP) as it is an opportunistic nosocomial organism. The current study was to find out the antibiotic resistance pattern of Acinetobacter baumannii, its phenotype and the genetic characterization of Metallo-β-Lactamase (MBL) genes that are responsible for carbapenem resistance.
Methods: One hundred and fifty Carbapenem resistant Acinetobacter baumannii (CRAB) specimens were isolated and PCR amplification of organism specific blaOXA-51gene was performed and antibiotic susceptibility was checked. Phenotypic susceptibility analysis was performed by Modified Hodge Test (MHT) and Imipenem-EDTA Double Disc Synergy Test (IMP-EDTA DDST). The carbapenemases and MBL producing genes were amplified by PCR.
Results: CRAB showed high resistance against piperacillin/tazobactam (99.3%), cefepime and ceftazidime (99.3% each), amikacin (91.3%), ciprofloxacin (96.7%) and levofloxacin (96.7%). Only one isolate showed resistance to colistin. The isolates positive for both MHT and DDST (n=70) were further characterized to detect metallo-β-lactamase genes. Molecular characterization revealed the presence of blaOXA-51 gene in all tested isolates (100%) followed by bla-VIM 89%, bla-OXA-23 64%, respectively and so on. Few genes coexisted with each other including blaVIM, blaOXA 23, blaOXA 51 and blaNDM-1. None of the isolate was found positive for blaIMP gene.
Conclusion: It is concluded that CRAB isolates exhibited a high rate of resistance towards antimicrobials because of the presence of drug-hydrolyzing enzymes such as carbapenemmases and MBLs. This is among the rare study reported recently indicating CRAB isolates co-harboring many resistant genes are very difficult to treat. There is a dire need to develop novel antibiotics against resistant A. baumannii to minimize its prevalence. Moreover, it is recommended that colistin treatment in the clinical settings should be continuously monitored to prevent the development of resistance.
Keywords: Acinetobacter baumannii; Carbapenem resistance; Metallo-beta-Lactamases; Resistant genes
Introduction![]()
Acinetobacter species are universal, free-living bacilli found in sewage, soil, water and contaminated food [1]. Acinetobacter are gram negative coccobacilli, non-motile, glucose non-fermenter, non-fastidious, catalase positive and oxidase negative. The genus contains pathogenic species causing significant nosocomial infections [2]. Acinetobacter baumannii (A. baumannii) has the ability to survive in the low-moist environment and also to develop resistance against antimicrobials [3]. Scientific literature highlights the Acinetobacter as principal pathogen of hospital acquired infections however, fewer reports also document infections in general populations [4,5]. Prolonged hospitalization, venous catheters, nursing home residence, and an impaired immune system are some risk factors for A. baumannii infection [6]. It causes infections like pneumonia, wound sepsis, septicemia, urinary tract infections, endocarditis meningitis, and endocarditis [7].
ESKAPE bacterial pathogens are the notorious critters known for their difficult to treat properties. They are S. aureus, E. faecium, K. pneumoniae, A. baumannii, P. aeruginosa, and Enterobacteriaceae family. These bacteria have a higher risk of developing antimicrobial resistance. Among this ESKAPE group, A. baumannii is the worst to treat due to its unique antibiotic resistance pattern[8]. A. baumannii isolates are becoming more resistant to many antimicrobials, including beta-lactams, aminoglycosides, and fluoroquinolones posing serious public health concerns [9]. Carbapenem is an antibiotic of class of β-lactam and is the recent resort therapeutics for the control of bacterial infections particularly, associated with A. baumannii[10]. In recent years, the reports suggested the increase in resistance of A. baumannii strains to carbapenem. Carbapenems are the drugs to treat these infections [11]. High mortality rate (50%) associated to carbapenem resistant bacteria has been reported [12]. Carbapenemase is one of the most frequent enzymes reported in carbapenem resistant A. baumannii[13]. Carbapenem resistance in A. baumannii is because of the production of class B, C and D carbapenemases [14,15]. Due to the production of OXA-type carbapenemase and Metalloβ-Lactamases (MBLs) most Acinetobacter spp. develop the carbapenem resistance [16,17]. Among OXA-type carbapenemases bla OXA-23 like, bla OXA-40 like, bla OXA-58 like and bla OXA-51 like are commonly reported, while bla OXA-51 like β-Lactamase is used for species identification and is intrinsically resistant to A. baumannii [18,19]. Various metallo-β-lactamase genes such as IMP, VIM, SPM, KPC, OXA, and NDM have been reported in A. baumannii conferring AMR to carbapenems [13]. Antimicrobial resistance is a major threat in developing countries leading to greater number of treatment failure in nosocomial infections[20]. By 2050, antimicrobial resistance is expected to cause 10 million deaths if the current situation continues [21].
Keeping in consideration the antimicrobial resistance and a raised level of nosocomial infections, in current study antibiotic resistance pattern, phenotypic characterization and Molecular identification, and sequencing of carbapenemase producing genes bla IMP, bla VIM, bla OXA 23 and bla OXA-24, bla OXA-51, bla OXA-58 and NDM-1 from CRAB were studied.
Methods![]()
The study was jointly conducted by Institute of Microbiology, University of Veterinary and Animal Sciences, (UVAS) Lahore, Pakistan and Institute of molecular biology and biotechnology department of University of Lahore (UOL). Strains of A. baumannii were collected from various pathological laboratories and tertiary care hospitals in Lahore including Chughtai Institute of Pathology from April 2021 to April 2022. The design of the study was approved by the ethical review committee of University of Lahore (UOL).
Isolation of A. baumannii
A total of 150 Carbapenem resistant A. baumannii strains were isolated from various clinical specimens including blood, pus, wound swabs, sputum, tracheostomy swabs, tracheal secretions, cerebrospinal fluid, CVP tip, bronchoalveolar lavage, drain fluid, and tissues.
Identification of A. baumannii
At initial, isolates were cultured on blood agar medium and MacConkey agar and were incubated at 37˚C for 24-48 hours. Different biochemical tests like Gram staining, catalase test, oxidase test and Analytical Profile Index (API) were performed for identification purpose [22, 24].
Antibiotic resistance patterns of Carbapenem resistant Acinetobacter baumannii determination
Antibiotic susceptibility testing of A. baumannii was checked by Kirby Bauer Disc Diffusion method as mentioned by CLSI [25]. Antibiotic discs contained cefepime (30 µg), ceftazidime (30 µg), Imipenem (10 µg), Meropenem (10 µg), Amikacin (30 µg), Gentamicin (10 µg), Tobramycin (10 µg), Doxycycline (30 µg), Ciprofloxacin (5 µg), Levofloxacin (5 µg), Trimethoprim sulphate (25 µg). They were placed onto the MHA plate and incubated at 37°C for 24 hours. After 24 hours zones of inhibition around antibiotic discs were evaluated and declared as sensitive, intermediate and resistant as per the guidelines of clinical and laboratory institute (CLSI). The antibiotic susceptivity testing of colistin was carried out by Minimum Inhibitory Concentration (MIC) by broth microdilution method as per Clinical Laboratory Standard Institute CLSI using Muller Hinton Broth [26].
Phenotypic assays for the determining β-lactamases (Carbapenemases & Metallo-β-Lactamase)
The detection of Carbapenemase producing A. baumannii was performed by Modified Hodge test as mentioned earlier by Amjad et al [27]. According to them ATCC Escherichia coli 25922 equivalents to 0.5 McFarland was swabbed on Muller Hinton Agar. In the center of plate disc of meropenem 10 µg was placed. From the edge of the antibiotic disc to the edge of the plate the test organism was streaked and the incubated at 37°C for 24 hours. MHT positive test showed a clover leaf like indentation of Escherichia coli 25922 growing along the test organism growth streak within the disk diffusion zone after 24 hours.
The identification of Metallo-β-Lactamase producing A. baumannii was carried out by IPM-EDTA double disc synergy test according to a study done by Young el al [28]. Inoculum equivalent to 0.5 McFarland of A. baumannii was swabbed onto Muller Hinton Agar. A 10 µg of imipenem disc and a sterile blank disc were placed 10 mm apart from edge to edge. As a control another imipenem disc was placed far. A volume of 10 µL of 0.5M EDTA solution was put into the blank disc. After overnight incubation, the established zone diameter difference of ≥ 7 mm between imipenem disk and imipenem plus EDTA will be interpreted as EDTA synergy positive.
Molecular identification of Carbapenem resistance determinants
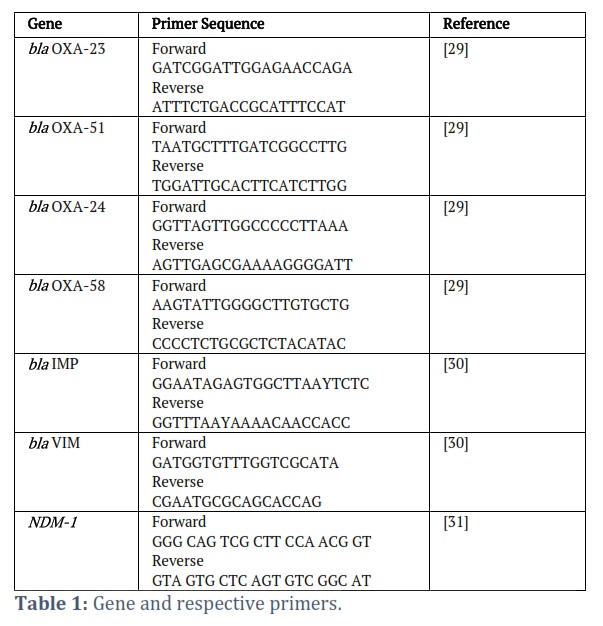
By PCR using gene specific primers for bla OXA-23, bla OXA-51, bla OXA-24, bla OXA-58, bla IMP, bla VIM and bla NDM-1 gene as shown in table 1. The characterization of Carbapenemase & MBL encoding genes in A. baumannii was performed. The primers were synthesized on order by Macrogen, Inc., Seoul Korea. Multiplex PCR was performed for bla-OXA genes. PCR conditions for bla-OXA genes and MBL encoding genes (bla IMP, bla VIM and bla NDM-1) were set as usual.
Sequencing analysis
Sequencing of amplified samples (bla OXA-23, bla OXA-24, bla OXA51, bla OXA-58, blaNDM-1, bla VIM) was done by services of Advance Biosciences International (ABI) Company. Sequences were analyzed by Chromas software and then got confirmed with the help of Basic Local Alignment Search Tool (BLAST). Nucleotide sequences were submitted to the Gen Bank for their accession numbers.
Statistical analysis
The clinical analysis of data was done by using SPSS, version 26. To find any possible association between demographic variables, specimens, isolates, antimicrobial resistance and genome of CRAB Chi-square or fisher exact test were used.
Results![]()
Identification and isolation of A. baumannii
One hundred and fifty Carbapenem resistant A. baumannii (CRAB) exhibiting the following morphological characteristics: Gram-negative short coccobacillus on gram staining, non-motile, non-pigmented, mucoid and domed shaped colonies on chocolate and blood agar, non-lactose fermenting colonies over MacConkey, were isolated. They appeared to be catalase positive and oxidase negative. A. baumannii were also identified by API 20 E. Further confirmation was done by presence of bla OXA 51 gene in the isolates.
Prevalence of CRAB from different wards
Out of 150 isolates, highest prevalence was observed from Medical ICU (28%) followed by Surgical ICU (18%), Surgical wards (16.6%) Pediatric ICU (16.6%), Medical ward (15.3%), and lowest was observed from Pediatric ward (5.3%).
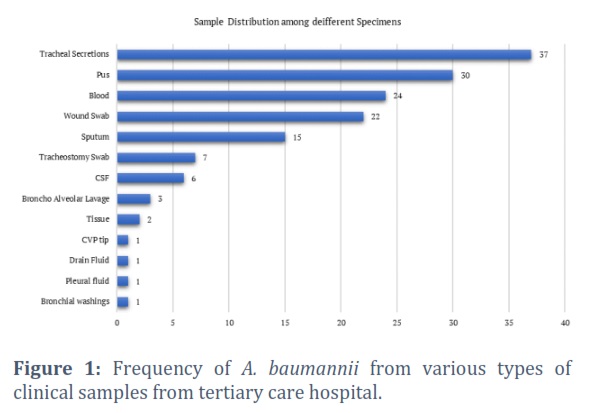
Prevalence of CRAB from different specimens
The maximum percentage of CRAB were isolated from tracheal secretions (24.7%), followed by pus (20.00%), blood (16.00%), wound swab (14.7%), sputum (10.00%), tracheostomy swab (4.70%), CSF (4.00%), alveolar lavage (2.00%), tissue samples (1.30%) and minimum percentage from bronchial washings (0.70%), pleural fluid (0.70%), drain fluid (0.70%) and CVP tip(0.70%) respectively Figure 1.
Prevalence of CRAB from different age groups
The maximum percentage of CRAB isolates were obtained from the patients of 21 to 40 years of age group (34.00%) followed by 41 to 60 years of age group (28.00%) and the minimum percentage of isolates were isolated from less than 01 years (11.33%) and 01 to 20 years age group (11.33%) respectively.
Frequency of CRAB from gender
The maximum percentage of CRAB were isolated from males (60.66%) as compared to females (39.33%) respectively.
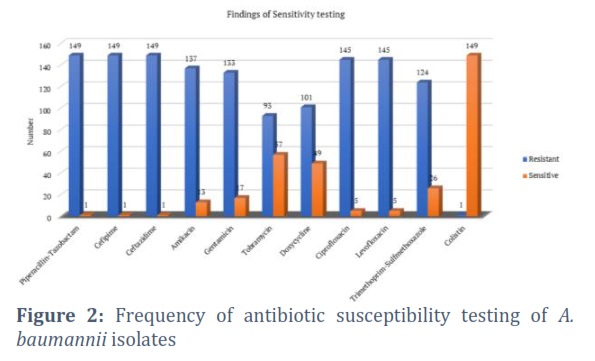
Antibiotic resistance pattern
Out of 150 CRAB isolates, highest level of resistance was found in piperacillin-tazobactam (99.30%), cefepime (99.30%), ceftazidime (99.30%), Ciprofloxacin (96.7%), levofloxacin (96.7%), amikacin (91.3%), gentamicin (88.7%), tobramycin (62%), trimethoprim-sulfamethoxazole (82.7%) and doxycycline (67.3%). Amongst all antibiotics only colistin (0.7%) showed better activity against CRAB respectively (Figure 2). All clinical isolates were found resistant to most antibiotic groups and were considered multi drug resistant.
Phenotypic characterization of metallo- β-Lactamase production and carbapenemase
All the isolates (n=150) were characterized phenotypically for production of Carbapenemase by Modified Hodge Test (MHT). The maximum number of isolates 143 (95%) were positive for Carbapenemase production. By double disc synergy test (DDST) the detection of metallo-β-Lactamase producing A. baumannii was. Out of 150 isolates, 74 (49.3%) were positive for metallo-β-Lactamase production.
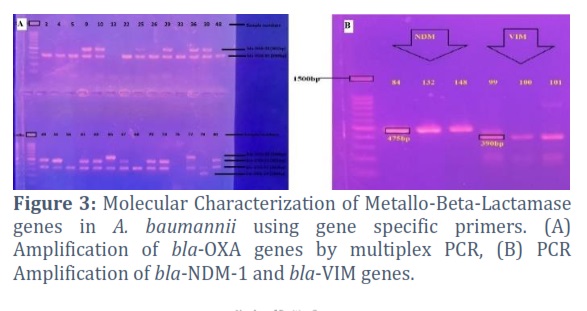
Molecular characterization of Metallo β-Lactamase gene
Seventy isolates that tested positive for both the Modified Hodge Test and the IPM-EDTA double disc synergy test were selected for further genetic characterization of carbapenem resistant genes. The MBL genes bla NDM-1, bla OXA-23, bla OXA-24, bla OXA-51, bla OXA-58, bla VIM and bla-IMP were amplified by using gene specific primers as seen in Figure 3.
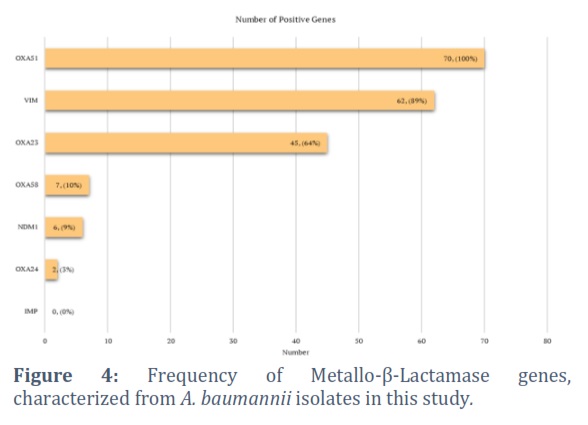
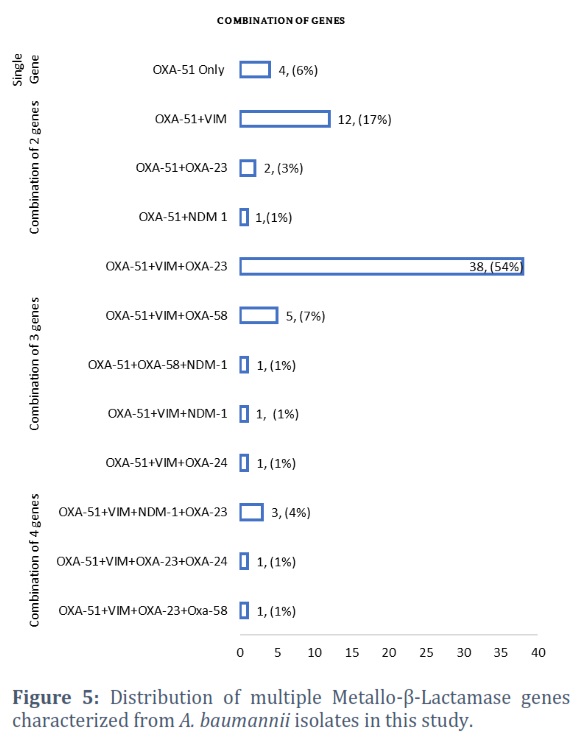
bla OXA 51 gene had the maximum rate of amplification and exhibited positive amplification for all 70 samples followed by bla VIM (62/70) 89%, bla OXA-23 (45/70) 64%, bla OXA-58 (7/70) 10%, bla NDM-1 (6/70) 9% and bla OXA-24 (2/70) 2.8%. None of the isolate was positive for bla IMP gene as shown in Figure 4. Furthermore, these genes coexisted with each other in combinations as well. The most common combination was a 3 gene combination in 38(54%) isolates harboring bla VIM, bla OXA 23 and bla OXA 51 genes. A combination of 4 genes occurred simultaneously in 3 (4%) isolates having bla VIM, bla OXA 23, bla OXA 51 and bla NDM-1 as shown in Figure 5.
Figures & Tables
β-Lactam antibiotics have been among the most effective medications used to treat bacterial infections in humans over past 60 years. Acinetobacter has developed as a significant disease class, posing ongoing hazards and problems to the global health care system [32-34]. In A. baumannii resistance to β-Lactams specially carbapenems and cephalosporins has been excessively seen globally and this is also the case in Pakistan.
The present study showed a high resistance pattern of different antibiotics towards carbapenem resistant A. baumannii isolated from various clinical specimens which revealed that our results are coinciding with the previous study in Egypt (98%), Greece (96.9%) and India (100%) [35-37]. The present study illustrates the prevalence of MBL producing A. baumannii 74/150 (49.3%) that is consistent with previous studies from Pakistan as well as from other countries. A similar study from Lahore, Pakistan reported that 63/112 (56.25%) of A. baumannii were MBL producers [38]. A study conducted in Iran showed a high prevalence 86/108 (86.86%) of MBL producing carbapenem resistant A. baumannii [39]. In Asian countries the incidence of MBL producing A. baumannii have been reported as 77% in 2019 in China [40]
In the present study bla OXA-51 was most prevailing 70/70(100%), followed by bla-VIM 62/70 (89%), bla-OXA 23 45/70 (64%), bla-OXA 58 7/70 (10%), bla NDM-1 6/70 (8.5%) and bla OXA-24 2/70 (2.8%). In this study None of isolate was positive for bla IMP gene. A study in Spain showed a 100% prevalence of bla OXA-51 in A. baumannii which is similar to our study [41].
In our study, these carbapenem resistant genes coexisted with each other in combinations as well. The most common combination was a 3 gene combination in 38(54%) isolates harboring bla VIM, bla OXA 23 and bla OXA 51 genes together. Majority of A. baumannii isolates were co-producers of class B and D carbapenemases harboring bla IMP, bla OXA 23 and bla NDM-1 in a study conducted in India [42]. Similar studies were previously reported in different countries [43-45]. In the current study a rise in resistance is seen among the A. baumannii isolates that is a major public health concern. As, the majority of isolates showed susceptibility to colistin indicating that colistin could play possible role in the control and treatment of carbapenem resistant A. baumannii [46].
This study possesses several shortcomings as well. The study was only done in Lahore, and the sample size was quite small. It is highly recommended that this research should be conducted on a broader scale and in other clinical settings throughout the country to obtain more of a valid susceptibility pattern against MDR and XDR A. baumannii, which will assist in controlling the transmission of infections that is caused by this deadly organism and will also be helpful for managing infectious diseases in a better way.
It is concluded that CRAB is major threat in hospitals of Pakistan and isolates exhibited a high rate of resistance to antimicrobials because of the presence of drug hydrolyzing enzymes, carbapenemases and MBLs. We also found that bla OXA-24, bla OXA-58, bla OXA-51, bla OXA-23, bla NDM-1, and bla VIM genes had not been widely reported in Pakistan. This study further concluded, CRAB isolates, co-harboring many resistant genes are very difficult to treat. There is a dire need to invent new antibiotics against resistant A. baumannii for reduction of its prevalence. Moreover, in order to prevent the development of resistance it is highly recommended that colistin treatment in the clinical settings should be continuously monitored. Understanding of genetic characterization and molecular epidemiology of A. baumannii to devise strategies for prevention and control of MDR infections are also necessary.
Competing Interest
The authors declare no conflict of interest.
Principal investigator, collection of data and Manuscript writing by Saadia Ijaz. Study conception and design by Farheen Ansari. Technical supervision and interpretation of results by Prof. Muhammad Nawaz. Sample and data collection by Karam Rasool. Technical guidance and final review by Prof. Aftab Anjum.
![]()
References
- Doughari HJ, Ndakidemi PA, Human IS, Benade S. Virulence factors and antibiotic susceptibility among verotoxic non O157: H7 Escherichia coli isolates obtained from water and wastewater samples in Cape Town, South Africa. African Journal of Biotechnology, (2011); 10(64): 14160-14168.
- Lin M-F, Lan C-Y. Antimicrobial resistance in Acinetobacter baumannii: From bench to bedside. World Journal of Clinical Cases: WJCC, (2014); 2(12): 787.
- Yu Y-S, Yang Q, Xu X-W, Kong H-S, Xu G-Y, et al. Typing and characterization of carbapenem-resistant Acinetobacter calcoaceticus–baumannii complex in a Chinese hospital. Journal of medical microbiology, (2004); 53(7): 653-656.
- Alfandari S, Gois J, Delannoy P-Y, Georges H, Boussekey N, et al. Management and control of a carbapenem-resistant Acinetobacter baumannii outbreak in an intensive care unit. Medecine et maladies infectieuses, (2014); 44(5): 229-231.
- Szabó S, Feier B, Capatina D, Tertis M, Cristea C, et al. An overview of healthcare associated infections and their detection methods caused by pathogen bacteria in Romania and Europe. Journal of Clinical Medicine, (2022); 11(11): 3204.
- Fishbain J, Peleg AY. Treatment of Acinetobacter infections. Clinical infectious diseases, (2010); 51(1): 79-84.
- Towner K. Clinical importance and antibiotic resistance of Acinetobacter spp.: Proceedings of a symposium held on 4-5 November 1996 at Eilat, Israel. Journal of medical microbiology, (1997); 46(9): 721-746.
- Gonzalez-Villoria AM, Valverde-Garduno VJJop. Antibiotic-resistant Acinetobacter baumannii increasing success remains a challenge as a nosocomial pathogen, (2016); 2016.
- Andrade SS, Jones RN, Gales AC, Sader HS. Increasing prevalence of antimicrobial resistance among Pseudomonas aeruginosa isolates in Latin American medical centres: 5 year report of the SENTRY Antimicrobial Surveillance Program (1997–2001). Journal of antimicrobial chemotherapy, (2003); 52(1): 140-141.
- Lott H (2023) Molecular mechanisms underpinning intraspecies co-infections with multiple Acinetobacter baumannii strains: Macquarie University.
- Girija SA, Priyadharsini JV, Paramasivam A. Prevalence of carbapenem-hydrolyzing OXA-type β-lactamases among Acinetobacter baumannii in patients with severe urinary tract infection. Acta Microbiologica et Immunologica Hungarica, (2020); 67(1): 49-55.
- Bratu S, Mooty M, Nichani S, Landman D, Gullans C, et al. Emergence of KPC-possessing Klebsiella pneumonia in Brooklyn, New York: epidemiology and recommendations for detection. Antimicrobial agents and chemotherapy, (2005); 49(7): 3018-3020.
- Cornaglia G, Riccio M, Mazzariol A, Lauretti L, Fontana R, et al. Appearance of IMP-1 metallo-β-lactamase in Europe. The Lancet, (1999); 353(9156): 899-900.
- Héritier C, Poirel L, Lambert T, Nordmann P. Contribution of acquired carbapenem-hydrolyzing oxacillinases to carbapenem resistance in Acinetobacter baumannii. Antimicrobial agents and chemotherapy, (2005); 49(8): 3198-3202.
- Quale J, Bratu S, Landman D, Heddurshetti R. Molecular epidemiology and mechanisms of carbapenem resistance in Acinetobacter baumannii endemic in New York City. Clinical infectious diseases, (2003); 37(2): 214-220.
- Thomson JM, Bonomo RA. The threat of antibiotic resistance in Gram-negative pathogenic bacteria: β-lactams in peril! Current opinion in microbiology, (2005); 8(5): 518-524.
- Amudhan MS, Sekar U, Kamalanathan A, Balaraman S. blaIMP and blaVIM mediated carbapenem resistance in Pseudomonas and Acinetobacter species in India. The Journal of Infection in Developing Countries, (2012); 6(11): 757-762.
- Cicek AC, Saral A, Iraz M, Ceylan A, Duzgun A, et al. OXA-and GES-type β-lactamases predominate in extensively drug-resistant Acinetobacter baumannii isolates from a Turkish University Hospital. Clinical Microbiology and Infection, (2014); 20(5): 410-415.
- Kusradze I, Diene SM, Goderdzishvili M, Rolain J-M. Molecular detection of OXA carbapenemase genes in multidrug-resistant Acinetobacter baumannii isolates from Iraq and Georgia. International journal of antimicrobial agents, (2011); 38(2): 164-168.
- Ayukekbong JA, Ntemgwa M, Atabe ANJAR, Control I. The threat of antimicrobial resistance in developing countries: causes and control strategies, (2017); 6(1): 1-8.
- O’neill JJRAR. Antimicrobial resistance: tackling a crisis for the health and wealth of nations, (2014); Review on Antimicrobial Resistance
- Tripathi N, Sapra A. Gram staining, (2020).
- Chauhan A, Jindal T, Chauhan A, Jindal TJMMfE, Food, Analysis P. Biochemical and molecular methods for bacterial identification, (2020); 425-468.
- Whitman WB Bergey’s manual of systematics of Archaea and Bacteria. Chapter: Book Name. 2015 of publication; 410; Wiley Online Library.
- Clinical, Institute LS (2017) Performance standards for antimicrobial susceptibility testing. Clinical and Laboratory Standards Institute Wayne, PA.
- CLSI C. M100-S25: Performance Standards for Antimicrobial Susceptibility Testing. Twenty-Fifth Informational Supplement, (2012).
- Amjad A, Mirza I, Abbasi S, Farwa U, Malik N, et al. Modified Hodge test: A simple and effective test for detection of carbapenemase production. Iranian journal of microbiology, (2011); 3(4): 189.
- Yong D, Lee K, Yum JH, Shin HB, Rossolini GM, et al. Imipenem-EDTA disk method for differentiation of metallo-β-lactamase-producing clinical isolates of Pseudomonas spp. and Acinetobacter spp. Journal of clinical microbiology, (2002); 40(10): 3798-3801.
- Woodford N, Ellington MJ, Coelho JM, Turton JF, Ward ME, et al. Multiplex PCR for genes encoding prevalent OXA carbapenemases in Acinetobacter spp. International journal of antimicrobial agents, (2006); 27(4): 351-353.
- Ellington MJ, Kistler J, Livermore DM, Woodford N. Multiplex PCR for rapid detection of genes encoding acquired metallo-β-lactamases. Journal of Antimicrobial Chemotherapy, (2007); 59(2): 321-322.
- Perry JD, Naqvi SH, Mirza IA, Alizai SA, Hussain A, et al. Prevalence of faecal carriage of Enterobacteriaceae with NDM-1 carbapenemase at military hospitals in Pakistan, and evaluation of two chromogenic media. Journal of Antimicrobial Chemotherapy, (2011); 66(10): 2288-2294.
- Vrancianu CO, Pelcaru CF, Alistar A, Gheorghe I, Marutescu L, Popa M, et al. Escaping from ESKAPE. Clinical significance and antibiotic resistance mechanisms in Acinetobacter baumannii: A review. Biointerface Research in Applied Chemistry, (2021); 11(1): 8190–8203.
- Kaleem F, Usman J, Hassan A, Khan A. Frequency and susceptibility pattern of metallo-beta-lactamase producers in a hospital in Pakistan. The Journal of infection in developing countries, (2010); 4(12): 810-813.
- Evans BA, Hamouda A, Abbasi SA, Khan FA, Amyes SG. High prevalence of unrelated multidrug-resistant Acinetobacter baumannii isolates in Pakistani military hospitals. International journal of antimicrobial agents (Print), (2011); 37(6): 580-581.
- Vijayakumar S, Mathur P, Kapil A, Das BK, Ray P, et al. Molecular characterization & epidemiology of carbapenem-resistant Acinetobacter baumannii collected across India. The Indian journal of medical research, (2019); 149(2): 240.
- Nowak J, Zander E, Stefanik D, Higgins PG, Roca I, et al. High incidence of pandrug-resistant Acinetobacter baumannii isolates collected from patients with ventilator-associated pneumonia in Greece, Italy and Spain as part of the MagicBullet clinical trial. Journal of Antimicrobial Chemotherapy, (2017); 72(12): 3277-3282.
- Benmahmod AB, Said HS, Ibrahim RH. Prevalence and mechanisms of carbapenem resistance among Acinetobacter baumannii clinical isolates in Egypt. Microbial Drug Resistance, (2019); 25(4): 480-488.
- Anwar M, Ejaz H, Zafar A, Hamid H. Phenotypic detection of metallo-beta-lactamases in carbapenem resistant Acinetobacter baumannii isolated from pediatric patients in Pakistan. Journal of pathogens, (2016); 2016.
- Fallah F, Noori M, Hashemi A, Goudarzi H, Karimi A, et al. Prevalence of blaNDM, blaPER, blaVEB, blaIMP, and blaVIM genes among Acinetobacter baumannii isolated from two hospitals of Tehran, Iran. Scientifica, (2014); 2014.
- Huang Z-Y, Li J, Shui J, Wang H-C, Hu Y-M, et al. Co-existence of bla OXA-23 and bla VIM in carbapenem-resistant Acinetobacter baumannii isolates belonging to global complex 2 in a Chinese teaching hospital. Chinese medical journal, (2019); 132(10): 1166-1172.
- Ruiz M, Marti S, Fernandez-Cuenca F, Pascual A, Vila J. High prevalence of carbapenem-hydrolysing oxacillinases in epidemiologically related and unrelated Acinetobacter baumannii clinical isolates in Spain. Clinical microbiology and infection, (2007); 13(12): 1192-1198.
- Sharma S, Banerjee T, Yadav G, Kumar AJFiC, Microbiology I. Susceptibility profile of blaOXA-23 and metallo-β-lactamases co-harbouring isolates of carbapenem resistant Acinetobacter baumannii (CRAB) against standard drugs and combinations, (2023); 121068840.
- Zhao F, Liu H, Yao Y, Zhang L, Zhou Z, et al. Description of a Rare Pyomelanin-Producing Carbapenem-Resistant Acinetobacter baumannii Strain Coharboring Chromosomal OXA-23 and NDM-1, (2022); 10(4): e02144-02122.
- Anane YA, Apalata T, Vasaikar S, Okuthe GE, Songca SJIjom. Molecular detection of carbapenemase-encoding genes in multidrug-resistant Acinetobacter baumannii clinical isolates in South Africa, (2020); 2020.
- Sen B, Joshi SJJoam. Studies on Acinetobacter baumannii involving multiple mechanisms of carbapenem resistance, (2016); 120(3): 619-629.
- Kallel H, Bahloul M, Hergafi L, Akrout M, Ketata W, et al. Colistin as a salvage therapy for nosocomial infections caused by multidrug-resistant bacteria in the ICU. International journal of antimicrobial agents, (2006); 28(4): 366-369.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0