

Full Length Research Article
The correlation between atrophic gastritis and Helicobacter pylori infection in patients referred to Shohadaye Ashayer Hospital in Khorramabad
Ghobad Abangah1, Ahmed Hjazi2, Rana Sherdil Amin3, Ghadeer Sabah Bustani4, Rosario Mireya Romero-Parra5, Rahman S. Zabibah6, Mosayeb Moradniani7, Mahsa Yousefpour Marzbali8, Mohamad Reza Nazer9*, Masoumeh Tahmasebi10
Adv. life sci., vol. 10, no. 3, pp. 375-380, September 2023
*– Corresponding Author: Mohamad Reza Nazer (mnazer@gmail.com)
Authors' Affiliations
2. Department of Medical Laboratory Sciences, College of Applied Medical Sciences, Prince Sattam bin Abdulaziz University, Al-Kharj – Saudi Arabia
3. Sharif Medical and Dental College Lahore , Pakistan – Iran
4. College of Dentistry, The Islamic University, Najaf – Iraq
5. Department of General Studies, Universidad Continental, Lima – Perú
6. Medical Laboratory Technology Department, College of Medical Technology, The Islamic University, Najaf – Iraq
7. Department of Internal Medicine, Lorestan University of Medical Sciences, Khorramabad – Iran
8. Research Center for Immunodeficiencies, Children’s Medical Center, Tehran University of Medical Sciences – Iran
9. Department of Infectious Diseases and Tropical Medicine, School of Medicine, Isfahan University of Medical Sciences, Isfahan – Iran
10. School of Medicine, Emam Khomeini Hospital, Ilam University of Medical Sciences, Ilam – Iran
[Date Received: 29/10/2022; Date Revised: 10/06/2023; Date Published Online: 30/09/2023; Date Updated: 06/09/2025]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Helicobacter pylori and atrophic gastritis are both known as risk factors for gastric cancer. The purpose of this study is to investigate the prevalence of Helicobacter pylori infection in patients with atrophic gastritis. In addition to being aware of the prevalence of this infection, it is crucial to eliminate this bacterium due to its carcinogenicity.
Methods: In this descriptive-cross-sectional study, all patients referred to the endoscopy unit of Shohadaye Ashayer Hospital in Khorramabad city for endoscopy during 2015–2016 were included. Patients with atrophic gastritis were classified as patients, while those without the condition were classified as the control group. Then, the frequency of H. pylori infection in patients with atrophic gastritis and people without atrophic gastritis was investigated. After sample collection, the primary data was entered into the SPSS software version 22 for analysis.
Result: The collected results showed that 41 % patients did not have H. pylori and 59% patients had H. pylori. The population over 50 years old had the highest age frequency in the study subjects, while the female group had the majority gender group. As a result, the frequency of H. pylori in the antrum area was higher than in other locations in both endoscopy and pathology, but it was not statistically significant (P value >0.05). While the frequency was higher, the overall difference across all locations was not statistically significant, but the association between H. pylori and atrophy in the antrum was statistically significant when evaluated more specifically. 54.1% of those who had endoscopy-discovered atrophy also had severe atrophy. H. pylori was found in the antrum in 50% of cases, and in 61.1% of cases when the pathology showed atrophy. This finding was statistically significant (P value <0.05).The incidence of reporting atrophy was 2.8 times higher in the age group of over 50 compared to those under 20. H. pylori was detected in 56.4% of people over 50 who had atrophy; that was statistically significant.
Conclusion: According to the results, there is a significant risk of developing atrophic gastritis in patients with H. pylori, and among females, those over 50 years old have the highest frequency of occurrence.
Keywords: Atrophic gastritis; Helicobacter pylori; Endoscopy; Iran
Introduction![]()
Chronic diseases such as gastric cancer is the second most prevalent cancer among cancer patients in terms of mortality, which is the fourth most common disease in terms of incidence [1, 2]. The risk of chronic diseases and gastric cancer is different among countries and individuals [3]. About 80% of gastric cancer cases occur in Asia [4]. The progression stages of gastric cancer, known as Correa’s cascade, have the following intermediate stages or precancerous lesions: gastritis, atrophic gastritis, intestinal metaplasia, dysplasia, and finally gastric cancer [5-7]. Gastric cancer has two types, intestinal and diffuse. Although the pathogenesis of the diffuse type is not well known, the pathogenesis of the intestinal type is associated with precancerous lesions [8]. Atrophic gastritis is a long-term inflammatory condition of the gastric mucosa that impairs the secretory capacity of the stomach and is associated with an increased risk of developing gastric cancer. The variables that impact the severity and spread of atrophic gastritis define the association between H. pylori and gastric cancer [9]. Both atrophic gastritis and H. pylori are recognized as risk factors for stomach cancer. Atrophic gastritis affects about one-third of H. pylori infection patients, and Helicobacter removal has been shown to reverse this precancerous lesion [10]. In general, the prevalence of atrophic gastritis is higher in countries with high prevalence of Helicobacter pylori and gastric cancer [9]. H. pylori is a spiral microaerophilic Gram-negative bacterium that colonizes in the mucosa of the human digestive tract [11]. According to reports, the prevalence of this infection ranges from 30% in the United States to 90% in developing countries as Iran [12-14].World Health Organization (WHO) considers Helicobacter pylori as a first-class carcinogen in the occurrence of gastric cancer, so that the eradication of H. pylori is effective in preventing the development of precancerous lesions [15]. Colonization of bacteria in the gastric mucosa leads to chronic inflammation that creates a carcinogenic sequence and causes gastric cancer after a few decades [5]. Helicobacter is responsible for 80% of atrophic gastritis cases and the association of this infection with atrophic gastritis or intestinal metaplasia increases the risk of gastric cancer 5-6 times [7].Considering this important role, the aim of this study is to investigate the frequency of Helicobacter pylori infection in patients with atrophic gastritis. In addition to being aware of how common this infection is, the necessary strategies for eradicating this organism ought to take its carcinogenicity into consideration.
Methods![]()
All patients who were referred to the endoscopy unit of Shohadaye Ashayer Hospital in Khorramabad for endoscopy during 2015–2016 were analyzed in this cross-sectional descriptive study. All those in whom atrophic gastritis was confirmed were regarded as patients, whereas the others were regarded as the control group. Patients whose pathology reports were not available were excluded from the study. Small mucosal vessels can be recognized when atrophic gastritis is present because it appears in endoscopy as hypopigmented and bright areas. Atrophy can be limited to a specific area (focal) or several areas (multifocal) or involve the entire gastric mucosa (diffuse). After retrieving the endoscopic report for these patients from the hospital database, the pathology report for these patients was requested from the public and private pathology laboratories in the city. A checklist that is particular to the same patient is used to record demographic data such as age and sex, gastric atrophy information such as the location and severity (focal, multifocal, diffuse) based on the endoscopic report, and Helicobacter information based on the pathology report. The frequency of H. pylori infection was then compared between individuals with and without atrophic gastritis. Following sample collection, the fundamental data was input into the SPSS version 22 software, which then used descriptive statistics (mean, standard deviation, and frequencies), Contingency table, the chi-square test, and logistic regression. A significance level of less than 0.05 was taken into consideration.
Results![]()
According to the data, 2889 patients (55.8%) had H. pylori, while 2285 patients (44.2%) did not. People over 50 years old were the most frequent age group, and females were the most frequent gender among the study subjects. As a result, the frequency of H. pylori in the antrum area was higher than in other locations in both endoscopy and pathology, but it was not statistically significant (P value>0.05). 54.1% of those who had endoscopy-discovered atrophy also had severe atrophy. In 50% of cases, H. pylori was detected in the antrum, and in 61.1% of cases when the pathology showed atrophy. This result was statistically significant (P value <0.05).
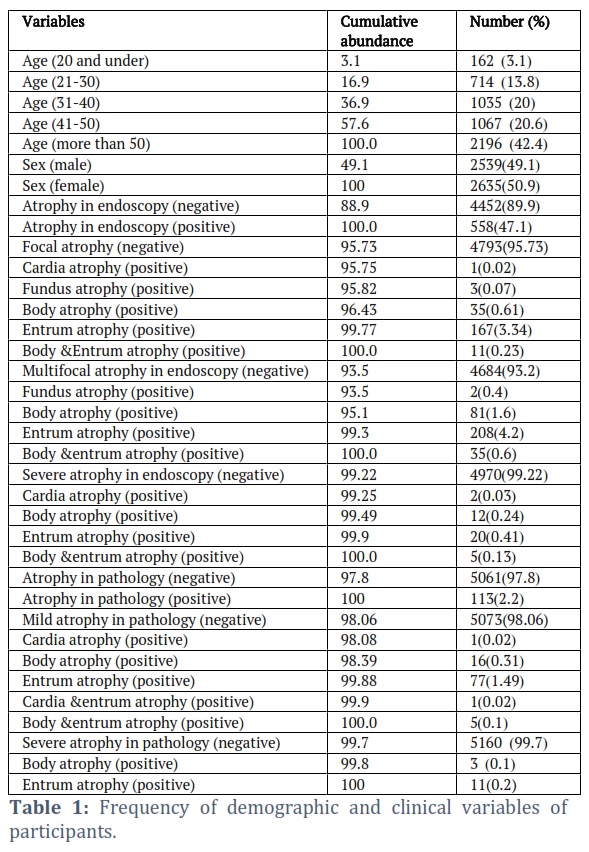
The probability of observing atrophy was 2.8 times higher in the age group of people over 50 compared to those under 20. H. pylori was only detected in 56.4% of people who were older than 50 and had atrophy, which was statistically significant. The frequency of demographic and clinical variables of participants under investigation is given in Table 1.
5010 people were investigated in this study. The average age of the patients was 48.3 ± 17.3, and the minimum age was 11 and the maximum was 95 years. Table 1 displays the frequency of demographic and clinical characteristics. H. pylori was detected in 3053 patients (59%) but not in 2121 (41%) of the cases. The highest frequency of age in the study subjects was related to the group over 50 years old and the highest frequency according to gender was related to the female group. The antrum region had the highest prevalence of atrophy in both endoscopy and pathology.Table2 displays the prevalence of H. pylori in various areas in both with and without atrophy cases in both endoscopy and pathology. The results showed the frequency of H. pylori in the antrum area was higher than in other areas in both endoscopy and pathology, but it was not statistically significant (P value >0.05).
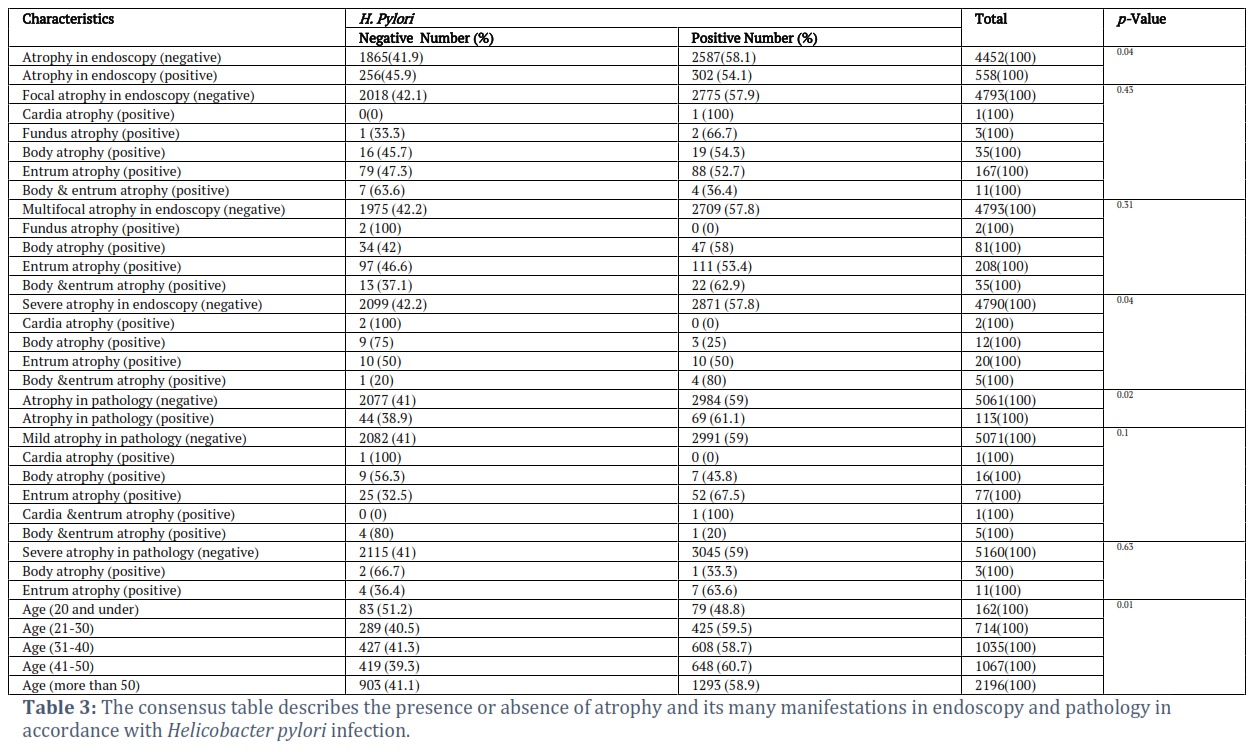
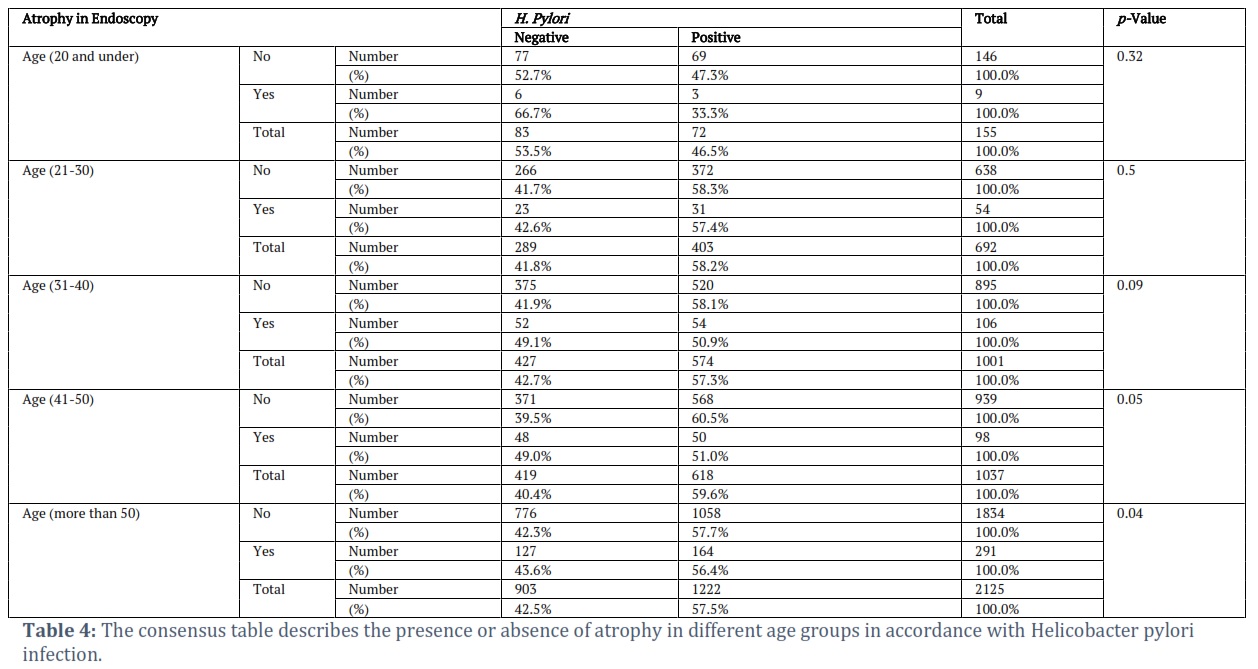
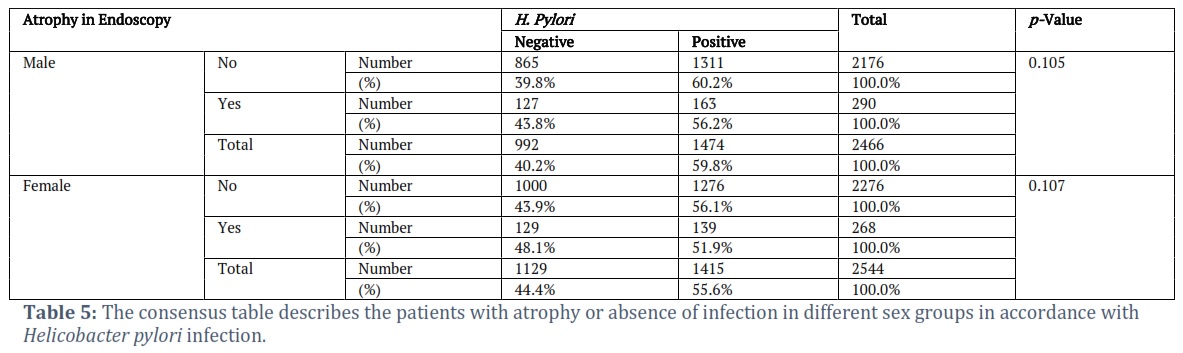
Table. 3 shows the prevalence of H. pylori in endoscopy and pathology samples from individuals with or without atrophy. It has shown 54.1% of those with endoscopic atrophy, 50% of those with severe antrum atrophy, and 61.1% of those with pathological atrophy all had H pylori, which was statistically significant (P value <0.05). Additionally, logistic regression was used to control confounders, and it was shown that, when other complicating factors were held constant, there was a 2.92-fold higher probability of endoscopic atrophy in people who had H. pylori than in people who did not (95% CI: 1.92–4.97). In addition, patients with H. pylori had a 14.3 times higher chance of having atrophy in their pathology than those without it (95% CI: 5.3–9.5). In the age group of patients over 50 compared to those under 20, the frequency of observing atrophy was 2.8 times higher (95% CI: 1.3–4.5). As shown in the Table 4, H. pylori was detected in 56.4% of patients over 50 years old who had atrophy, which was statistically significant. Although there was atrophy in both the male and female groups, and there were more than 50% pylori infections, the results in the above table demonstrate that they were not statistically significant.
Figures & Tables

Various studies on the correlation between H. pylori infection and atrophic gastritis have been carried out in different countries. For example, in the study of Chen and his colleagues in China, 3969 patients with atrophic gastritis were examined, of which 21.01% had Helicobacter pylori infection. Also, 92.33% of patients infected with Helicobacter had experienced inflammation in the gastric mucosa at the same time [20]. Furthermore, in a study that took place in Cameroon during 2013-2014, 79 patients who were diagnosed with gastritis based on histological findings were examined. The results revealed that Helicobacter pylori infection was present in 71.2% of patients with atrophic gastritis and was absent in 28.8% of patients [8]. Moreover, Darnindro et al., investigated 69 patients with Helicobacter in the case group and 71 people in the control group in Indonesia in 2014. According to the study, there was more mild and moderate atrophy and intestinal metaplasia in the Helicobacter group than in the control group. Additionally, 62.3% of Helicobacter patients and 12.7% in the control group reported having chronic active gastritis [21]. The outcomes of these studies support our findings about the association between H. pylori infection and the occurrence of atrophic gastritis.
In 2007, a study has been well established to investigate the correlation between H. pylori infection, gastritis, and mucosal atrophy [2]. Also,In Bhutan in 2010, 381 patients with dyspepsia were screened, and 71.1% of them were found to have Helicobacter pylori infections. 341 patients had atrophy in the antrum and 140 patients had atrophy in the corpus in addition to the antrum. This study demonstrated a strong correlation between atrophic gastritis of the stomach and antrum and Helicobacter infection [3].Later in 2015, Myint conducted research on 252 dyspepsia patients in Myanmar, who had endoscopy and biopsy. In this study, 48% of participants had Helicobacter. Atrophic gastritis affected the antrum in 54.7% of patients and the corpus in 12.6% of individuals. In this study, the group with Helicobacter infection had much more atrophy and more severe atrophy than the non-infected group [23]. A study published in 2012 by Leja et al. Included the evaluation of 3564 individuals from the general community in Latvia. H. pylori infection was determined in these individuals through the serological examination, and 79.21% of the population had the infection. Pepsinogen levels showed that 40.52 percent of the participants under study had different levels of atrophy, indicating a significant prevalence of Helicobacter and atrophic gastritis in Latvia [24].
The use of natural compounds is recommended for the treatment of digestive factors and diseases [25-28] because they are rich in natural antioxidants [27-30]. These findings show that patients with H. pylori have a considerably greater risk of developing atrophic gastritis. Also, individuals over 50 years old have the highest incidence of this condition, and females are more likely than males to have it.
According to the results, there is a significant risk of developing atrophic gastritis in patients with H. pylori, and while the frequency was highest in females over 50, the association between gender and atrophy was not statistically significant in this study.
Competing Interest
The authors declare that there is no conflict of interest.
Mosayeb Moradniani (Co-coresponding authors): Conception and design, Experimental Work, Analysis and interpretation of data, Rough Draft.
Mosayeb Moradniani: Supervision, Research Project Administration.
Ahmed Hjazi, Rana Sherdil Amin, Ghadeer Sabah Bustani, Rosario Mireya Romero-Parra, Rahman S. Zabibah: Analysis and Interpretation.
Mahsa Yousefpour Marzbali, Mohamad Reza Nazer: Final Draft, writing and Revision. Mahsa Yousefpour
Marzbali, Mohamad Reza Nazer: Final Draft and Revision.
Ghobad Abangah, Mahsa Yousefpour Marzbali, Mohamad Reza Nazer: Draft editing.
![]()
References
- Ilic M, Ilic I. Epidemiology of stomach cancer. World Journal of Gastroenterology, (2022); 28(12):1187.
- Chophel T, Tshering S, Dorji N, Tshomo U. Stomach cancer screening services of Bhutan. Indian Journal of Surgery, (2022); 23:1-6.
- Manouchehri N, Ghodsi S, Atri F, Sarraf P, Seyedi D, Valizadeh S. Effect of pretreatment of root dentin surface with cold atmospheric plasma on improving the bond strength of fiber post and resin cement: In vitro study. Clinical and Experimental Dental Research, (2023); 9(4): 653-660.
- Mohammed ZJ, Rasool KH, Ahmed MA. Relationship between Helicobacter pylori infections and vitamin D level and lipid profile in some obese Iraqi women. Caspian Journal of Environmental Sciences, (2021); 19(5): 801-807.
- Tokunaga M, Yoshikawa T, Boku N, Nishida Y, Tanahashi T, Yamada T, Haruta S, Etoh T, Hirahara N, Kawachi Y, Tsuji K. Impact of COVID-19 on gastric cancer treatment in Japanese high-volume centers: a JCOG stomach cancer study group survey. Surgery today, (2022); 52(2): 231-8.
- Suh M, Wikoff D, Lipworth L, Goodman M, Fitch S, Mittal L, Ring C, Proctor D. Hexavalent chromium and stomach cancer: a systematic review and meta-analysis. Critical Reviews in Toxicology, (2019); 49(2): 140-59.
- Yang L, Zheng R, Wang N, Yuan Y, Liu S, Li H, Zhang S, Zeng H, Chen W. Incidence and mortality of stomach cancer in China, 2014. Chinese Journal of Cancer Research, (2018); 30(3): 291.
- Nadeem H, Nawaz A, Nawaz A, Shams K, Mubarak B. Frequency of Helicobacter pylori Infections and Its Associated Risk Factors in Patients Attending Tertiary Care Hospital of Bhakkar, Pakistan. Advancements in Life Sciences, (2022); 9(3): 323-7.
- Shah SC, Piazuelo MB, Kuipers EJ, Li D. AGA clinical practice update on the diagnosis and management of atrophic gastritis: expert review. Gastroenterology, (2021); 161(4): 1325-32.
- Ghobadi E, Ghanbarimasir Z, Emami S. A review on the structures and biological activities of anti-Helicobacter pylori agents. European Journal of Medicinal Chemistry, (202); 223: 113669.
- Watari J, Chen N, Amenta PS, Fukui H, Oshima T, Tomita T, et al. Helicobacter pylori associated chronic gastritis, clinical syndromes, precancerous lesions, and pathogenesis of gastric cancer development. World Journal of Gastroenterology: WJG, (2014); 20(18): 5461.
- Lan HC, Chen TS, Li AFY, Chang FY, Lin HC. Additional corpus biopsy enhances the detection of Helicobacter pylori infection in a background of gastritis with atrophy. BMC gastroenterology, (2012); 12(1): 1.
- Öztekin M, Yılmaz B, Ağagündüz D, Capasso R. Overview of Helicobacter pylori Infection: Clinical Features, treatment, and nutritional aspects. Diseases, (2021); 9(4): 66.
- Charitos IA, D’Agostino D, Topi S, Bottalico L. 40 Years of Helicobacter pylori: a revolution in biomedical thought. Gastroenterology Insights, (2022); 12(2): 111-35.
- Siao D, Somsouk M. Helicobacter pylori: evidence-based review with a focus on immigrant populations. Journal of general internal medicine, (2014); 29(3): 520-8.
- Tshibangu-Kabamba E, Yamaoka Y. Helicobacter pylori infection and antibiotic resistance—from biology to clinical implications. Nature Reviews Gastroenterology & Hepatology, (2021); 18(9): 613-29.
- Moayyedi P, Wason C, Peacock R, Walan A, Bardhan K, Axon AT, et al. Changing patterns of Helicobacter pylori gastritis in long‐standing acid suppression. Helicobacter, (2000); 5(4): 206-14.
- Pan KF, Zhang L, Gerhard M, Ma JL, Liu WD, Ulm K, et al. A large randomised controlled intervention trial to prevent gastric cancer by eradication of Helicobacter pylori in Linqu County, China: baseline results and factors affecting the eradication. Gut, (2016); 65(1): 9-18.
- Correa P, Houghton J. Carcinogenesis of Helicobacter pylori. Gastroenterology, (2007); 133(2): 659.
- Chen S, Ying L, Kong M, Zhang Y, Li Y. The prevalence of Helicobacter pylori infection decreases with older age in atrophic gastritis. Gastroenterology research and practice, (2013).494783 ;
- Darnindro N, Syam AF, Handjari DR, Makmun D. Gastric Mucous Atrophy and Metaplasia in Patient with Helicobacter pylori Infection. The Indonesian Journal of Gastroenterology, Hepatology, and Digestive Endoscopy, (2015); 1(1): 13-6.
- Guindy A, Ghoraba H. A study of the Concordance between endoscopic gastritis and histological gastritis in nonulcer dyspeptic patients with and without Helicobacter pylori infection. Tanta Medical Sciences Journal, (2007); 2(2): 67-82.
- Myint T, Shiota S, Vilaichone RK, Ni N, Aye TT, Matsuda M, et al. Prevalence of Helicobacter pylori infection and atrophic gastritis in patients with dyspeptic symptoms in Myanmar. World Journal of Gastroenterology, (2015); 21(2): 620-7.
- Leja M, Cine E, Rudzite D, Vilkoite I, Huttunen T, Daugule I, et al. Prevalence of Helicobacter pylori infection and atrophic gastritis in Latvia. European journal of gastroenterology & hepatology, (2012); 24(12): 1410-7.
- Mandil O, Sabri H, Manouchehri N, Mostafa D, Wang HL. Root coverage with apical tunnel approach using propolis as a root conditioning agent: A case report with 2‐year follow‐up and review of the literature. Clinical and Experimental Dental Research, (2023); 9(4): 568-573.
- Baniesmaeeili SY, Akbarzadeh A, Riazi G, Abdollahi F, Niromand M. Effects of dietary Moringa oleifera leaf powder and ethanolic extract on expression function of immune genes of Litopenaeus vannamei. Aquatic Animals Nutrition, (2023); 9(1): 27-41.
- Salimi K, Atri F, Valizadeh S, Sahebi M, Ghodsi S, Manouchehri N. Influence of nonthermal argon plasma on the micro-shear bond strength between resin cement and translucent zirconia. Journal of Conservative Dentistry, (2023); 26(3): 281.
- Manouchehri N. Most Important Medicinal Plants with Anti-Halitosis Property: an Overview. Journal of Biochemicals and Phytomedicine, (2023); 2(1):1-2.
- Kakeshian S, Shirali S, Savari A, Najafzadehvarzi H, Zakeri M. Alterations in histological structure, blood estrogen and progesterone levels after oral administration of garlic extract in yellowfin seabream (Acanthopagrus latus). Aquatic Animals Nutrition, (2022); 8(2): 1-10.
- Manouchehri N. A Review of the Most Widely Used Medicinal Plants in the Treatment of Dental and Oral Disorders and Diseases, (2022); 1(1): 3–7.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0