

Review Article
Research Progress of Applied Anatomy of Labia Minora in Plastic Surgery
Rizwan Ali, Jinghong Xu, Rui Lei*
Adv. life sci., vol. 11, no. 1, pp. 01-06, February 2024
*– Corresponding Author: Rui Lei (11418264@zju.edu.cn)
Authors' Affiliations
[Date Received: 17/05/2023; Date Revised: 01/08/2023; Date Published: 25/02/2024]
Abstract![]()
Introduction
Methods
Discussion
Conclusion
References
Abstract
Cosmetic labiaplasty is focusing on the deliberate alteration of external genitalia without medical reasons. It highlights the growing understanding of diverse genital anatomy, suggesting that the labia minora innervation contributes to sexual arousal and pleasure. The measurement of female vulva structure is crucial for aesthetic standards and surgical planning. Past research gathered labia minora measurements from various countries, races, and age groups. As women’s expectations for vulva appearance increase, the demand for labia minora plastic surgery rises, emphasizing the importance of safety and effectiveness. To enhance surgical planning, this article addresses the histology, anatomy, data measurement, aesthetics, blood supply, and nerve innervation of the labia minora, considering both its morphological beauty and functional requirements.
Keywords: Labia minora; Anatomy; Measurement; Blood and nerve supply; Plastic surgery
Introduction![]()
The field of female genital plastic surgery, including procedures like labiaplasty, has witnessed a significant surge in popularity. In the United States alone, the number of labiaplasty procedures rose by an impressive 870% over a span of less than a decade—from 2142 procedures in 2011 to 18,813 procedures in 2021 [1,2]. Nevertheless, it is important to note that these statistics may not fully capture the total number of procedures performed, as gynecologists also carry out such surgeries [3]. This upward trend in cosmetic genital surgeries is not limited to the United States but has been observed globally. Several factors contribute to this increase, encompassing functional, sexual, and appearance-related concerns among individuals, the widespread availability of online information, the prevalent exposure to photographs on the internet, practices such as depilation, negative societal comments, and cultural influences [4-11].
The labia minora is located inside the labia majora and outside the vestibule. It is a pair of thin skin folds, soft and red in color, smooth and hairless. The outer inter-labial groove separates it from the labia majora. The lateral folds of the labia minora form the foreskin above the clitoris, while their medial parts form the clitoral frenulum below the glans, where the lower ends of the left and right labia minora meet to form the labial frenulum. The size and shape of the labia minora vary, and they can appear asymmetrical or split [12].
The classical anatomy description of the female vulva is relatively straightforward. However, due to the growing demand for labia minora plastic surgery, both domestic and foreign scholars have increasingly focused on various aspects of the labia minora. This article aims to provide a comprehensive discussion based on the latest research literature regarding the histology, fine anatomy, data measurement techniques, and aesthetics of the labia minora. By synthesizing these research findings, our objective is to create a comprehensive reference guide for surgeons, enabling them to enhance their understanding of the labia minora. This knowledge will aid in developing effective surgical plans that address both the aesthetic preferences and functional needs of women seeking labia minora plastic surgery.
Methods![]()
Literature Search and Selection Criteria
In order to gather relevant information, a comprehensive literature search was conducted using PubMed and Google Web Browser. Key terms such as “anatomy of vulva,” “histology of labia minora,” “blood supply of labia minora,” “measurement data of labia minora,” “role of plastic surgery in vulva aesthetic,” “labiaplasty in different countries,” “labiaplasty of labia minora,” and “plastic surgery and labia minora” were utilized. The search results were carefully evaluated to ensure their relevance to the topic at hand. From the initial pool of literature, a total of 33 peer-reviewed research articles were selected for inclusion in this study.
Discussion![]()
Histological feature
The labia minora originate from the urogenital folds. The epidermis, which is a stratified squamous epithelium with papillary protrusions, contains melanocytes deposited at the base of the epithelium. The epidermis is thinner than the labia, and the degree of keratosis gradually weakens. From the inner third of the labia minora to the vestibule, the epithelium is a nonkeratinized mucosal tissue of endoderm origin. It consists of large, loose, moderately flattened cells that contain glycogen granules. Hart’s line delineates the transition between the keratinizing epithelium of the labia minora (embryologically derived from ectoderm) and the non-keratinizing epithelium of the vaginal vestibule (embryologically derived from endoderm)[13]. The subcutaneous tissue consists mainly of connective tissue and vascular erectile tissue. It lacks adipose tissue but contains a small amount of lymphocyte infiltration. There are abundant sebaceous glands and eccrine sweat glands but no hair follicles. Simultaneously with sexual arousal, the labia minora can become swollen due to hyperemia, and their thickness can increase by 1 to 3 times [14]. The labia minora tissue is rich in a large number of nerve endings and sensory receptors, such as genital nerve corpuscles, spherical corpuscles, tactile corpuscles, and ring corpuscles Therefore, it exhibits a high degree of sexual sensitivity [15,16]. Another study [17] demonstrated that the epithelium of the labia minora contains abundant estrogen receptors, which are closely related to the development of the labia minora.
Vulva measurement and aesthetic standards
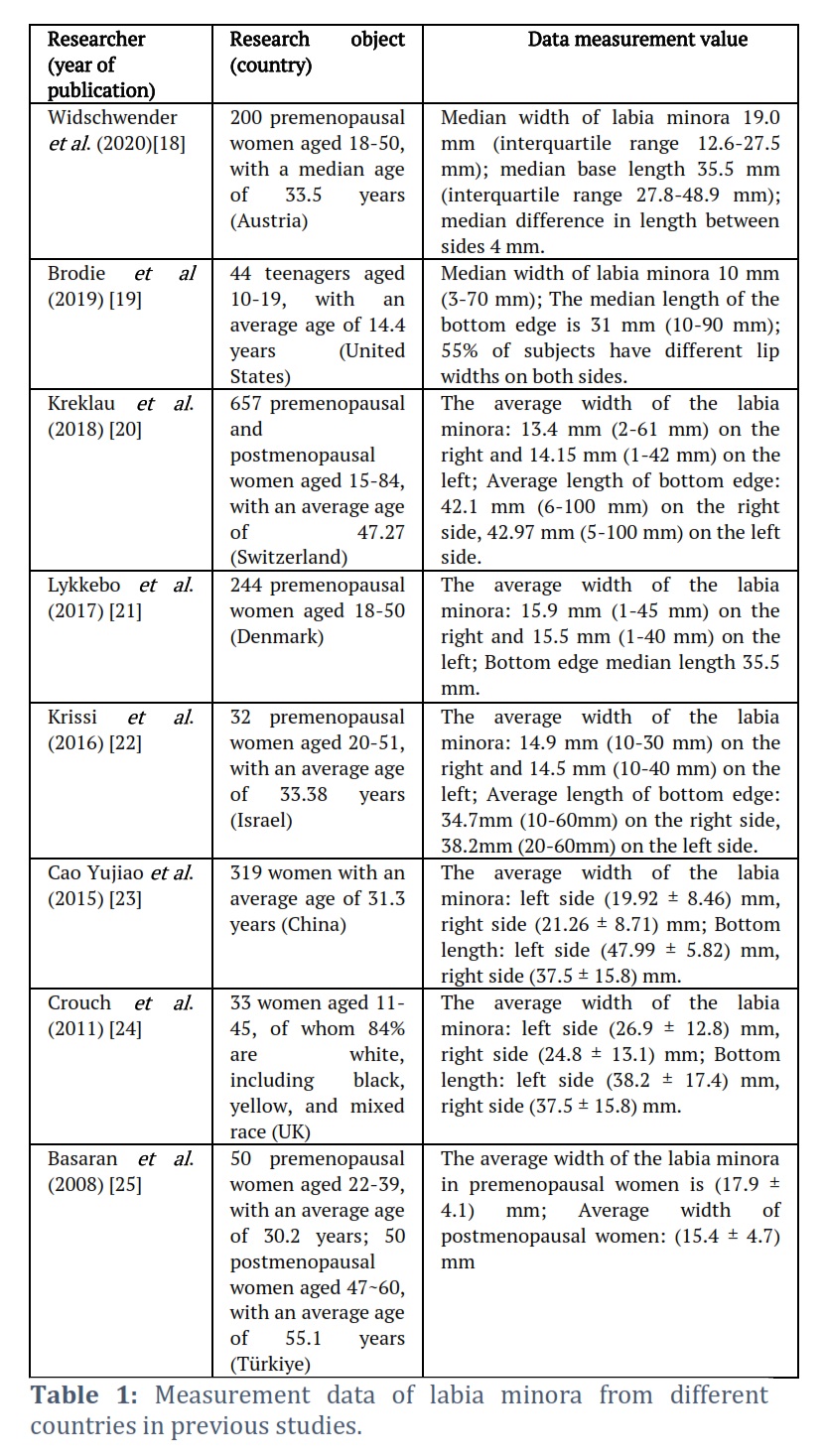
The measurement of the female vulva structure holds significant reference value for establishing aesthetic standards and designing surgical procedures. In previous research, the author selected measurements from scholars in various countries, different races, and different age groups to summarize the data on labia minora measurements (Table 1) [18-25]. Although there were differences in the inclusion and exclusion criteria, based on the aforementioned measurement results, it can be observed that there are substantial individual differences in the shape of the labia minora, with bilateral asymmetry being a common occurrence. Furthermore, there is a certain correlation between the shape of the female vulva and factors such as age, BMI, pregnancy, parity, and sexual activity. The labia minora may undergo atrophic changes after menopause [26]. In 1993, T Franco proposed a classification for the labia minora based on size, dividing them into four categories: type I, no hypertrophy, labia <2 cm; type II, labia size 2 to <4 cm; type III, labia size 4 to <6 cm; and type IV, labia ≥ 6 cm. Additionally, some opinions suggest that aesthetically pleasing labia minora are consistent with prepubertal morphological features, where the labia minora are covered by the labia majora when standing with legs together. Motakef et al., [27] classified the protruding distance of the labia majora from the outer edge of the labia minora into three grades: grade I (0-2 cm), grade II (>2-4 cm), and grade III (>4 cm). Smarrito et al., [28] discovered that different shapes of the labia minora caused different symptoms. They divided the labia minora into three types: type I, anterior 1/3 hypertrophy with a “flag-like” appearance, leading to unattractive appearance when wearing tights and discomfort in the perineal area; type II, hypertrophy in 1/3 of the labia minora, displaying an “oblique shape” and an overall bloated appearance; type III, hypertrophy in the posterior 1/3, giving a “round” appearance, causing more pain compared to types I and II, and the labia minora can obstruct the vaginal opening.
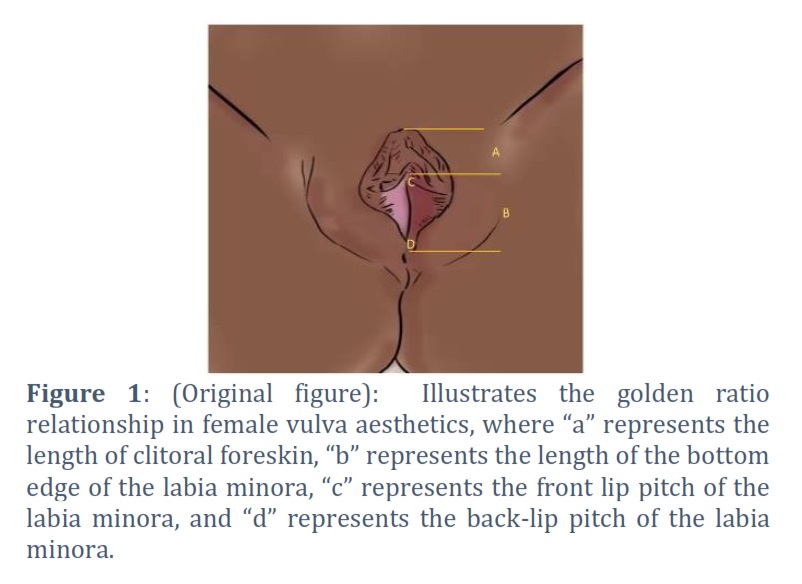
Some scholars [29,30] have described the ideal shape of the labia minora in terms of vulva structure proportions. Qiang et al., [18] combined vulva measurement data and proposed two golden ratios in the aesthetic standard of the labia minora (Figure 1): the length of the base of the labia minora to clitoral prepuce length = 1.618:1, and the distance between the labia minora and the posterior lip to the small anterior labial distance = 1.618:1. Frojo et al., [30], through analysis, found that the ratio of the width of the labia majora to the labia minora was 3:1, which obtained the highest score and was considered an ideal anatomical ratio.
Internationally, experts in the fields of gynecology, pediatrics, and plastic surgery have not yet reached a consensus on the aesthetic standards of the labia minora. The labia minora have physiological functions that include protecting the urethra and vaginal opening, preventing vaginal dryness, and guiding urine flow. The principle of surgery should be to achieve a postoperative appearance that is natural and beautiful, without compromising the normal physiological functions of the labia minora. Generally, a vertical distance from the midpoint of the labia minora width to the inter-labial groove of ≥10 mm is considered acceptable. The labia minora is a unique tissue in the body that cannot be easily reconstructed once excessive resection occurs. Therefore, it is crucial to adhere to the principle of “less is more” when performing resections [31]. Additionally, the principle of individualization should be followed, taking into full consideration the relative size and position of the labia minora, clitoral hood, and labia majora [32].
Characteristics of blood supply
In 1936, M Salmon et al., [33] discovered that the labia minora is perfused by arterioles perpendicular to the long axis of the labia. This discovery was made through the injection of a contrast medium in cadaveric cutaneous arteries, which revealed that these arterioles converged just below the labial rim. The posterior 2/3 of the labia minora receive perfusion from the internal pudendal artery, while the anterior 1/3 is perfused by the external pudendal artery. These two systems show a close connection at the junction between the front 1/3 and middle 1/3 of the labia. In 1985, Hwang et al., [34] conducted a study on 60 labia minora specimens, confirming that the branches of the external pudendal artery and the internal artery contribute to the blood supply of the labia minora and anastomose with each other to form six vascular arches.
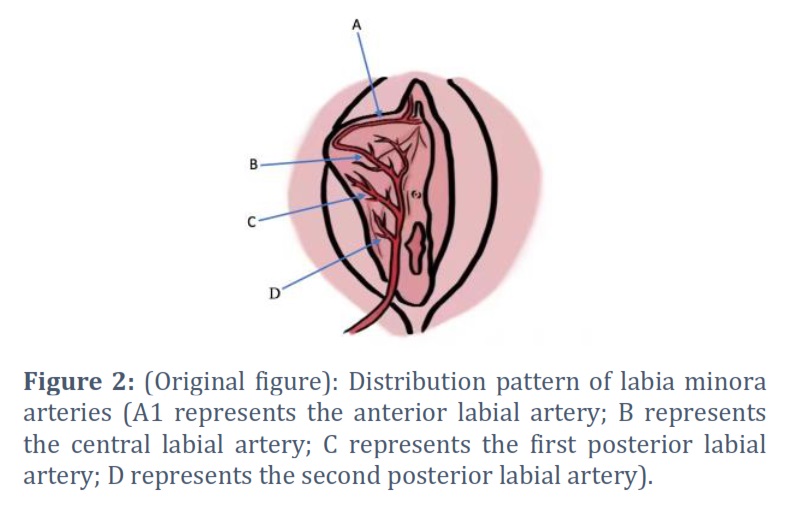
Georgiou et al., [35] utilized computed tomography and rotational angiography to identify the four main arteries of the labia minora. They constructed an arterial anatomical model (Fig. 2), which included a central artery in the relative center, referred to as the “Central labial artery.” Additionally, two branches were found behind the central labial artery and named the “first posterior labial artery” and “second posterior labial artery.” Another smaller branch was positioned in front of the “C” artery and named the “anterior labial artery.” Notably, the branches of the external pudendal artery, responsible for supplying the clitoris and the prepuce of the clitoris, form intricate connections with the branches of the internal pudendal artery on the mucosal surface of the most anterior part of the labia minora.
According to this study, the blood perfusion in the anterior part of the labia minora is relatively lower in comparison. As a result, performing a wedge resection in the frontal area can preserve a greater blood supply to the labia minora tissue.
Kaya et al., [36] assessed the vascular distribution of the labia minora by utilizing cold light sources during laparoscopic surgery to illuminate the outer surface of the labia minora. They found that the vascular distribution pattern may vary but generally conforms to the model proposed by Georgiou et al. However, the study encountered difficulty in distinguishing between arteries and veins.
Clarifying the blood supply characteristics of the labia minora is of great significance to prevent complications such as flap necrosis and incision dehiscence after labia minora reduction plastic surgery. Further studies with larger sample sizes and encompassing different shapes of labia minora are needed to advance our understanding.
Characteristics of nerve distribution
The labia minora not only has a rich blood vessel structure but is also an important sensitive tissue involved in sexual response. The effect of labia minora plastic surgery on the sensation of the labia minora, especially sexual experience, is still unclear [5,37]. This uncertainty has prompted researchers to further explore the innervation characteristics of the labia minora in order to guide the design and implementation of related procedures. Autopsy findings indicate that the female external genitalia are primarily innervated by the pudendal nerve. At the level of the superficial transverse muscle of the perineum, the pudendal nerve divides into deep and superficial branches. The superficial branch continues as the retro-labial nerve, providing innervation to the sensation of the labia minora [38]. However, the small nerve branches of the labia minora are difficult to further clarify using anatomical methods, leading scholars to turn to histological methods to analyze their innervation characteristics.
In 1975, L Malinovsky et al., [39] compared the sensory nerve endings in normal labia minora tissue and hypertrophic labia minora tissue and found no significant difference between the two. Schober et al., [15] performed argyrophilic staining on a portion of the labia minora tissue from 10 prepubertal women undergoing surgical resection due to labial fusion. They found the presence of high-density nerve bundles, with deeper staining observed on the inner side compared to the outer side. Therefore, it was concluded that the nerve endings of the labia minora are more abundant on the medial side. Ginger et al., [40] stained serial sections of labia minora specimens from 8 postmenopausal women and found that compared to the labia majora, the labia minora tissue had a large number of nerve fibers, and there was no significant difference in their distribution between the inner and outer surfaces along the long axis of the labia minora. The investigators believe that the presence of a central region with thick, myelinated nerve trunks accompanying the vascular structures within the labia minora serves as the anatomical basis for the engorgement and swelling of the labia minora during sexual arousal.
In a study by Kelishadi et al., [41], the density of sensory nerve distribution in the six anatomical regions of the labia minora was analyzed. The researchers found that the distribution of nerves in the labia minora was inconsistent. The nerve density of the innermost labia minora was slightly lower than that of the middle and outer parts, but there were no statistically significant differences in nerve density between anatomical subunits. Therefore, Kelishadi et al., believe that the labia minora has a consistent dense innervation throughout its anatomical structure. They suggest that regardless of whether marginal resection or wedge resection is performed, labial tissue with sensory nerve bundles will be preserved after surgery. Cao et al., [42] applied immunohistochemical staining to labia minora tissue from fresh cadavers and surgical specimens. They found no statistically significant difference in nerve counts between the inner and outer regions of the labia minora or in the distance between the main nerve bundles and the inner and outer epidermis. However, the current study’s tissue sections were not continuous, and the use of immunohistochemical staining makes it difficult to provide intuitive and accurate evidence regarding the shape and distribution of nerves in the labia minora.
Figures & Tables
The labia minora is an important structure of the female external genitalia and plays a significant role in sexual activity. The author conducted a review of the histology, blood supply, and innervation characteristics of the labia minora. Additionally, they analyzed data on female vulva measurements in various populations and discussed the classification and aesthetic standards of the labia minora. As the demand for female external genital plastic surgery continues to increase each year, there is a growing concern for its safety and effectiveness. Consequently, there is an urgent need to further clarify the intricate anatomical structure of the female genitalia, establish aesthetic standards, and provide a scientific basis for the development of related treatment procedures.
Conflict of Interest
The authors declare no conflict of interest.
Rizwan Ali and Jinghong Xu conceived the project. Jinghong Xu and Rui Lei supervised the project and provided guidance. All authors wrote, edited, and approved the final manuscript.
![]() References
References
- The Aesthetic Society. The Aesthetic Plastic Surgery National Databank Statistics 2021. Available at https://wwwtheaestheticsocietyorg/media/procedural-statistics, (Accessed July 26, 2023).
- Furnas HJ, Graw GJ, Cho MJ, Othman S, Graw B, et al. Safety in Female Genital Plastic Surgery. Plastic and Reconstructive Surgery, (2020); 146(4): 451e-463e.
- Sharp G, Maynard P, Hudaib AR, Hamori CA, Oates J, et al. Do Genital Cosmetic Procedures Improve Women's Self-Esteem? A Systematic Review and Meta-Analysis. Aesthetic Surgery Journal, (2020); 40(10): 1143-1151.
- Sorice-Virk S, Li AY, Canales FL, Furnas HJ. Comparison of Patient Symptomatology before and after Labiaplasty. Plastic and Reconstructive Surgery, (2020); 146(3): 526-536.
- Turini T, Weck Roxo AC, Serra-Guimarães F, Abreu ML, de Castro CC, et al. The Impact of Labiaplasty on Sexuality. Plastic and Reconstructive Surgery, (2018); 141(1): 87-92.
- Hamori CA. Aesthetic surgery of the female genitalia: labiaplasty and beyond. Plastic and Reconstructive Surgery, (2014); 134(4): 661-673.
- Lista F, Mistry BD, Singh Y, Ahmad J. The Safety of Aesthetic Labiaplasty: A Plastic Surgery Experience. Aesthetic Surgery Journal, (2015); 35(6): 689-695.
- Placik OJ, Devgan LL. Female Genital and Vaginal Plastic Surgery: An Overview. Plastic and Reconstructive Surgery, (2019); 144(2): 284e-297e.
- Dogan O, Yassa M. Major Motivators and Sociodemographic Features of Women Undergoing Labiaplasty. Aesthetic Surgery Journal, (2019); 39(12): Np517-np527.
- Earp BD, Steinfeld R. Genital Autonomy and Sexual Well-being. Current Sexual Health Reports, (2018); 107-17.
- Bucknor A, Chen AD, Egeler S, Bletsis P, Johnson AR, et al. Labiaplasty: Indications and Predictors of Postoperative Sequelae in 451 Consecutive Cases. Aesthet Surg J, (2018); 38(6): 644-653.
- Cohen Sacher B. The Normal Vulva, Vulvar Examination, and Evaluation Tools. Clinical Obstetrics and Gynecology, (2015); 58(3): 442-452.
- Yeung J, Pauls RN. Anatomy of the Vulva and the Female Sexual Response. Obstetrics and Gynecology Clinics of North America, (2016); 43(1): 27-44.
- Puppo V. Embryology and anatomy of the vulva: the female orgasm and women's sexual health. European Jounal of Obstetrics and Gynecology Reproductive Biology, (2011); 154(1): 3-8.
- Schober J, Cooney T, Pfaff D, Mayoglou L, Martin-Alguacil N. Innervation of the labia minora of prepubertal girls. Jounal Pediatric and Adolescent Gynecology, (2010); 23(6): 352-357.
- Martín-Alguacil N, Aardsma N, Litvin Y, Mayoglou L, Dupré C, et al. Immunocytochemical characterization of pacinian-like corpuscles in the labia minora of prepubertal girls. Journal of Pediatric and Adolescent Gynecology, (2011); 24(6): 353-358.
- Martin-Alguacil N, Pfaff DW, Kow LM, Schober JM. Oestrogen receptors and their relation to neural receptive tissue of the labia minora. BJU International, (2008); 101(11): 1401-1406.
- Widschwendter A, Riedl D, Freidhager K, Abdel Azim S, Jerabek-Klestil S, et al. Perception of Labial Size and Objective Measurements-Is There a Correlation? A Cross-Sectional Study in a Cohort Not Seeking Labiaplasty. Journal of Sexual Medicine, (2020); 17(3): 461-469.
- Brodie K, Alaniz V, Buyers E, Caldwell B, Grantham E, et al. A Study of Adolescent Female Genitalia: What is Normal? Journal of Pediatric and Adolescent Gynecology, (2019); 32(1): 27-31.
- Kreklau A, Vâz I, Oehme F, Strub F, Brechbühl R, et al. Measurements of a 'normal vulva' in women aged 15-84: a cross-sectional prospective single-centre study. Bjog An International Journal of Obstetrics and gynaecology, (2018); 125(13): 1656-1661.
- Lykkebo AW, Drue HC, Lam JUH, Guldberg R. The Size of Labia Minora and Perception of Genital Appearance: A Cross-Sectional Study. Journal of Lower Genital Tract Disease, (2017); 21(3): 198-203.
- Krissi H, Ben-Shitrit G, Aviram A, Weintraub AY, From A, et al. Anatomical diversity of the female external genitalia and its association to sexual function. European Journal of Obstetrics & Gynecology and Reproductive Biology, (2016); 19644-47.
- Cao Yujiao, Li Qiang, Zhou Chuande, Li Fengyong, Li Senkai, et al. A preliminary study on the measurement of external genitalia in women undergoing gynecological cosmetic surgery in China. Chinese Journal of Clinical Obstetrics and Gynecology, (2015); 16 (4): 333-336. 曹玉娇, 李强, 周传德, 李峰永, 李森恺, et al. 针对我国妇科美容手术女性外阴测量的初步研究. 中国妇产科临床杂志, (2015); 16(4): 333-336.
- Crouch NS, Deans R, Michala L, Liao LM, Creighton SM. Clinical characteristics of well women seeking labial reduction surgery: a prospective study. Bjog, (2011); 118(12): 1507-1510.
- Basaran M, Kosif R, Bayar U, Civelek B. Characteristics of external genitalia in pre- and postmenopausal women. Climacteric : the journal of the International Menopause Society, (2008); 11416-421.
- Wei Shuyi Basic and clinical research related to female breast and vulva rejuvenation: (2018) Peking Union Medical College. 魏蜀一 (2018). 魏蜀一 (2018) 女性乳房与外阴年轻化的相关基础与临床研究: 北京协和医学院.
- Motakef S, Rodriguez-Feliz J, Chung MT, Ingargiola MJ, Wong VW, et al. Vaginal labiaplasty: current practices and a simplified classification system for labial protrusion. Plastic and Reconstructive Surgery, (2015); 135(3): 774-788.
- Smarrito S. Classification of Labia Minora Hypertrophy: a retrospective study of 100 patient cases. Journal of Plastic, Reconstructive and Aesthetic Surgery Open, (2017); 13.
- Qiang S, Li FY, Zhou Y, Li Q. Golden Section in Vulva. Plastic and Reconstructive Surgery Global Open, (2020); 8(5): e2844.
- Frojo G, Kareh AM, Probst KX, Rector JD, Plikaitis CM, et al. Defining Ideal External Female Genital Anatomy via Crowdsourcing Analysis. Aesthetic Surgery Journal, (2022); 42(5): 505-515.
- Female Reproductive Surgery Branch of China Plastic Surgery Association Expert consensus on plastic surgery of Labia minora (2020 version). Chinese Journal of Practical Gynecology and Obstetrics, (2020); 36 (10): 968-970. 中国整形美容协会女性生殖整复分会. 小阴唇整形术专家共识(2020年版). 中国实用妇科与产科杂志, (2020); 36(10): 968-970.
- Yang E, Hengshu Z. Individualized Surgical Treatment of Different Types of Labia Minora Hypertrophy. Aesthetic Plastic Surgery, (2020); 44(2): 579-585.
- Salmon M Artères de la peau. Chapter: Book Name. 1936 of publication; Masson et cie Paris.
- Hwang WY, Chang TS, Sun P, Chung TH. Vaginal reconstruction using labia minora flaps in congenital total absence. Annals of Plastic Surgery, (1985); 15(6): 534-537.
- Georgiou CA, Benatar M, Dumas P, Chignon-Sicard B, Balaguer T, et al. A Cadaveric Study of the Arterial Blood Supply of the Labia Minora. Plastic and Reconstructive Surgery, (2015); 136(1): 167-178.
- Kaya AE, Dogan O, Yassa M, Basbug A, Çalışkan E. A Novel Technique for Mapping the Vascularity of Labia Minora Prior to Labiaplasty: Cold Light Illumination. Geburtshilfe und Frauenheilkdunde, (2018); 78(8): 775-784.
- Placik OJ, Arkins JP. A Prospective Evaluation of Female External Genitalia Sensitivity to Pressure following Labia Minora Reduction and Clitoral Hood Reduction. Plastic and Reconstructive Surgery, (2015); 136(4): 442e-452e.
- Pauls RN. Anatomy of the clitoris and the female sexual response. Clinical Anatomy, (2015); 28(3): 376-384.
- Malinovský L, Sommerová J, Martincík J. Quantitative evaluation of sensory nerve endings in hypertrophy of labia minora pudendi in women. Acta Anatomica (Basel), (1975); 92(1): 129-144.
- Ginger VA, Cold CJ, Yang CC. Structure and innervation of the labia minora: more than minor skin folds. Female Pelvic Medicine and Reconstructive Surgery, (2011); 17(4): 180-183.
- Kelishadi SS, Omar R, Herring N, Tutela JP, Chowdhry S, et al. The Safe Labiaplasty: A Study of Nerve Density in Labia Minora and Its Implications. Aesthetic Surgery Journal, (2016); 36(6): 705-709.
- Cao Y, Li F, Li S, Zhou Y, Li Q. A preliminary observational study on the vascular, nerve, and lymphatic anatomy and histology of the labia minora from cadaveric and surgical samples. International Urogynecology Journal, (2021); 32(5): 1169-1176.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0