

Metadata Analysis
Effect of Laughter Therapy on Depression among Middle-Aged Women: A Systematic Review and Meta-Analysis
Shannastaniar Aisya Adif1,2ˠ, Muhammad Abdullah3ˠ, Shih-Hsien Lin4,5,6, Huan-Fang Lee7*
Adv. life sci., vol. 11, no. 1, pp. 268-275, February 2024
*– Corresponding Author: Huan-Fang Lee (eamonn0330@gmail.com)
ˠ – Authors contributed equally.
Authors' Affiliations
2. STIKES Wira Medika Bali, Denpasar – Indonesia
3. Taiwan International Graduate Program in Interdisciplinary Neuroscience, National Cheng Kung University and Academia Sinica, Taipei – Taiwan
4. Department of Psychiatry, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University – Taiwan
5. Institute of Behavioral Medicine, College of Medicine, National Cheng Kung University – Taiwan
6. Clinical Medicine Research Center, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University – Taiwan
7. Department of Nursing, College of Medicine, National Cheng Kung University – Taiwan
[Date Received: 25/12/2022; Date Revised: 08/12/2023; Date Published: 25/02/2024]
Editorial Expression of Concern:
18 May 2025: Following publication of this paper, the internal audit (consequent to concerns on quality raised by Web of Science) notified Advancements in Life Sciences about missing record of the Turnitin Originality / AI Reports. By this Editorial Expression of Concern, we alert the scientific community of the errors as we reconcile the records.
Editorial Note:
28 May 2025: Missing record of the Turnitin Originality / AI Reports has been reconciled by conducting fresh analyses as per the editorial policy. Expression of concern is hereby revoked.
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Laughter therapy, known for its health benefits, has become a popular treatment for psychological conditions such as depression over the last ten years. The effectiveness of laughter therapy may differ with the cause of depression and the age of patients. No systematic reviews or meta-analyses have focused on the impact of laughter therapy on middle-aged women's depression. This study aimed to evaluate the effect of laughter therapy on depression in middle-aged women.
Methods: Randomized controlled trials (RCTs) or quasi-experimental studies on laughter therapy were included in this systematic review and meta-analysis which compared to the control group. The systematic review included English and non-English articles that were searched in CINAHL, MEDLINE, Cochrane Library, and EMBASE electronic databases. Search terms included laugh, qigong, laughter therapy, humor, yoga, intervention, depression, middle age, menopause, and women. The article screening process was conducted by four authors independently and finally agreed upon by all. This systematic review and meta-analysis were reported according to the PRISMA guidelines. JBI critical appraisal tools were used to assess the quality of inclusion studies. The risk of bias was assessed using the risk of bias in non-randomized studies – of Interventions (ROBINS-I) assessment tool.
Results: A total of 3102 studies were examined, and two publications (two quasi-experimental studies) were included. Studies were included and evaluated by the inclusion and exclusion criteria. The results indicated a significant decrease in depression among middle-aged women.
Conclusion: Laughter therapy demonstrated cost-effectiveness and exhibited no adverse effects in middle-aged women, making it a viable option for promoting health and reducing depression among middle-aged women.
Keywords: Laughter Therapy; Depression; Middle-Aged Women; Meta-Analysis
Introduction![]()
Depression is one of the major psychiatric diseases which may exacerbate other mental disorders [1,2], and affects an estimated 3.8% of the world population. According to the World Health Organization, approximately 280 million people have depression, with a prevalence of 5% in adults and 5.8% in people older than 60 years [3]. Aging is one of the contributing factors to depression in both men and women. Studies have reported that the prevalence of depression increases with age in women as compared to men [4]. The higher prevalence of depression in aging women may be due to multiple factors such as economic dependency, caregiving, financial strains, marital status (widowhood/living alone), and hormonal changes [4-6]. Middle age in women is associated with dynamic hormonal changes due to the event of menopause.
Menopause is a natural part of life that impacts every woman as aging ensues [7]. It has been reported that menopause increases the susceptibility to depression 2–5 times [8]. A decreased level of estrogen negatively modulates the brain neurotransmitter systems that are associated with mood and psychological well-being. For example, the disruptions of dopaminergic and serotonergic systems which are the most important systems related to the pathophysiology of depression have been reported in relation to estrogen level attenuation [5]. Along with neurophysiological changes, other bodily changes which are associated with menopause include vasomotor changes, night sweats, dyspareunia, hot flashes, and vaginal dryness, all of which negatively affect sleep and contribute to depression [9].
Due to the unique pattern of contributing factors, previous researchers have reported unique challenges in managing depression in middle-aged women. For example, hormonal therapies (i.e., estrogen and analogues) have been used to compensate for age and menopause-related fluctuations of sex hormones. Even though estrogen remains the first line of treatment for vasomotor changes, some non-hormonal therapies have been suggested earlier to tackle challenges associated with perimenopausal, postmenopausal, and middle-aged depression in women [10]. Non-hormonal therapies include psychoactive substances such as antidepressants, anti-anxiety therapies, mood stabilizers, and anticonvulsant medications. Hormonal and non-hormonal medicinal substances used as antidepressant therapies have a multitude of related adverse effects, including cardiogenic adverse events, cancer, loss of libido, insomnia, and suicide [11]. These adverse effects are also shared by increasing age and menopause. Furthermore, most of the patients relapse after treatment and rehabilitation [12]. Additional medicinal and non-medicinal options with less adverse effects and lower monetary expenditures are the need of time to overcome the problem of depression.
Multiple non-pharmacological treatment options are available for the treatment of depression, such as exercise [13], electroceuticals [14], nutritional additives [15], and laughter therapy [16]. Laughter therapy is one of the promising non-pharmacological treatments available currently [17]. Studies have shown positive effects of laughter therapy in different psychiatric ailments, including schizophrenia, anxiety, bipolar disorders, and depression among others [16,18]. Laughter therapy has been reported to recover the disrupted molecular integrity of various neurotransmitter systems and hormonal disturbances (i.e., cortisol) associated with depression [16]. It has shown tremendous efficacy in all age populations including the young, middle, and old ages. In middle-aged women previously, several studies have investigated the therapeutic effect of laughter therapy [19,20]. However, to our knowledge, there has not been a previous systematic review and meta-analysis conducted to assess the effect of laughter therapy on depression in middle-aged women. Thus, we aimed to find the effects of laughter therapy to treat depression in middle-aged women from 40-60 years old (age criteria according to WHO).
Methods![]()
Search strategy
The search strategy was elaborated and implemented to improve the quality of results and evidence synthesis according to Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. Population, Intervention, Comparison, and Outcome (PICO) were defined to ask the following question: “What is the effect of laughter therapy for depression among middle-aged women?”.
Four databases (CINAHL, MEDLINE, Cochrane Library, and EMBASE) were used to retrieve all the related topics in the field. All controlled vocabulary and synonyms were documented. The Boolean operators “AND” and “OR” were used to combine all MeSH terms, the controlled vocabulary, and free texts that have been verified by the medical librarian. Subsequently, a searching process was established (e.g., (("middle aged" OR "middle-aged") AND (women OR woman OR female OR mother OR lady OR lesbian* OR pregnan*) OR menopause*)) AND ((Gelototherapy) or (humour OR laugh*) AND (intervention or therapy* or qigong or yoga or meditation)) AND (depress* OR emotion* OR mood* OR "depression symptoms" ) in this analysis. The bibliographic software EndNote X9 was used to manage, organize, and store all the references.
Eligibility criteria
We included the studies in the systematic review if they were reported in English and non-English which involved (a) middle-aged women, 40–60 years old, healthy or with mild depression, undergoing (b) laughter therapy compared to (c) all forms of comparison or control groups, as assessed by (d) depression-related outcomes. The randomized controlled trial (RCT) and quasi-experimental study designs were the only ones included in this systematic review. All the non-primary studies and grey literatures, such as abstract conferences, theses and dissertations, editorials, literature reviews, clinical guidelines, and protocols were excluded. There was no restriction on publication year to increase the number of related studies. The comprehensive systematic search was done until August 2022.
Study selection
A blind, standardized procedure for assessing the eligibility of the studies was carried out by three reviewers (SAA, MA, and SHL). The title and abstract screening became the first process, then we proceeded to the full-text articles. In the first phase, all the disagreements and opinions on whether to include the article in the study or not were thoroughly assessed through the full-text analysis. A comprehensive discussion was held to resolve the disagreements and inconsistencies in data extraction between reviewers until consensus was obtained. The fourth reviewer, HFL, was responsible for reaching a consensus and doing an analysis to see if there were any conflicting decisions.
Data extraction
Study information on the authors, publication year, study design, characteristics of the participants, type of the intervention and control group, duration, frequency, outcome measurement tool, and main findings were extracted by 2 reviewers (SAA and MA) and independently double-checked by other reviewers (SHL and HFL) using data extraction in a Microsoft Word spreadsheet.
Outcome measures
All depression-related outcome studies were included in the systematic review and meta-analysis to explore the full review of the field. This was done for some reasons: (a) the limited or absence of a systematic review discussing the laughter therapy effect on depression and anxiety among the middle-aged women population so far, (b) the relatively high diversity of psychological outcomes which made the results likely heterogeneous and difficult to interpret.
Quality assessment
The JBI Level of Evidence for Effectiveness guidelines were used to define the grades of all inclusion studies. Risk of Bias assessment was performed using the ROBINS-I for quasi-experimental studies to ensure the quality of studies. The assessment was related to the following: (a) bias due to confounding; (b) bias in the selection of participants into the study; (c) bias in the classification of interventions; (d) bias due to deviations from intended interventions; (e) bias due to missing data; (f) bias in measurement of outcomes; (g) bias in selection of the reported result; then reported for the conclusion for overall bias (Low, Moderate, and Serious). Differences in bias assessment results were resolved through discussion among reviewers.
Analytic approach and data synthesis
A meta-analysis was performed using RevMan5 software for quasi-experimental to estimate the heterogeneity as the I2 statistic calculation and separate pooled effect size for both studies. Regarding the theory of [24]; the common interpretation for an I2 value of 0% shows no heterogeneity observed and higher values indicate higher heterogeneity observed within-subgroup (25%-low, 50%-moderate, 75%-high).
Results![]()
Literature search
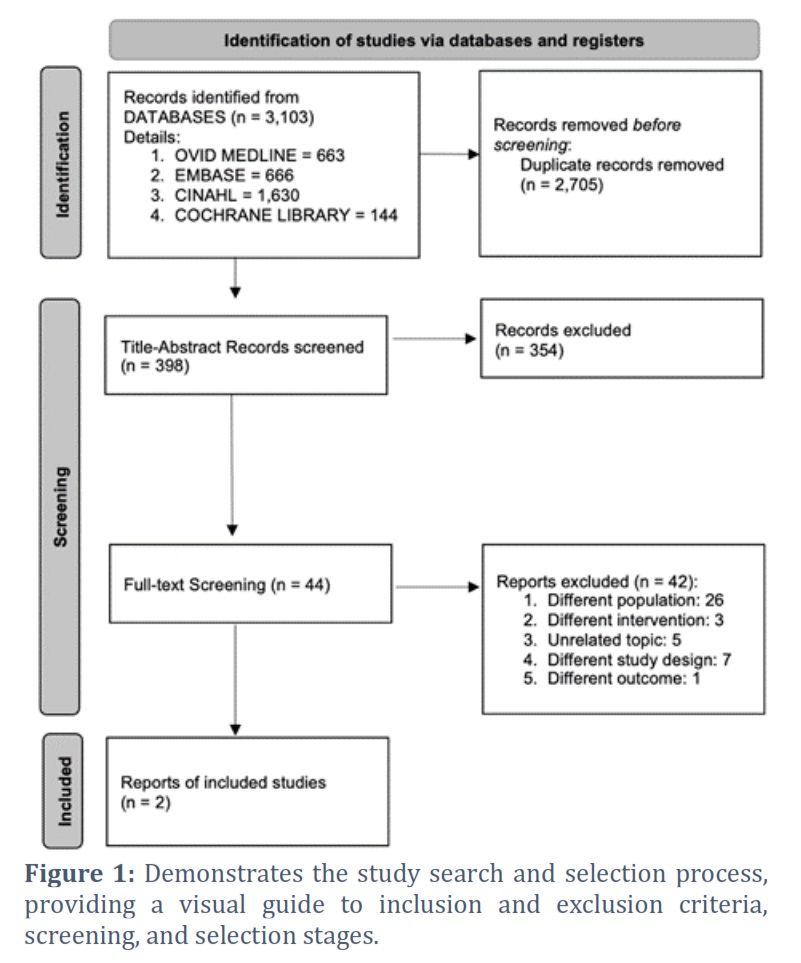
Initially, 3,102 potential articles were retrieved from 4 databases: CINAHL, MEDLINE, Cochrane Library, and EMBASE. After passing the screening procedures, two relevant Korean articles that matched the inclusion criteria for systematic review and meta-analysis were finally included. A total of 3,100 articles were excluded for reasons such as duplication, different intervention, different population, different outcome, unrelated topic, and full-text unavailable. The process of study selection using the PRISMA 2020 flow diagram is shown in Figure 1.
Risk of bias
Overall, the related studies were judged to have a low risk of bias using the ROBINS-I tool. No crucial information was missing from the studies. However, bias due to confounding, bias in the selection of participants, and bias due to missing data were moderately found in the article by Cha Mi-Yeon and Hong Hae-Sook [20]. Table 1 depicts the outcome of the risk of biased individual assessments.
Study characteristics
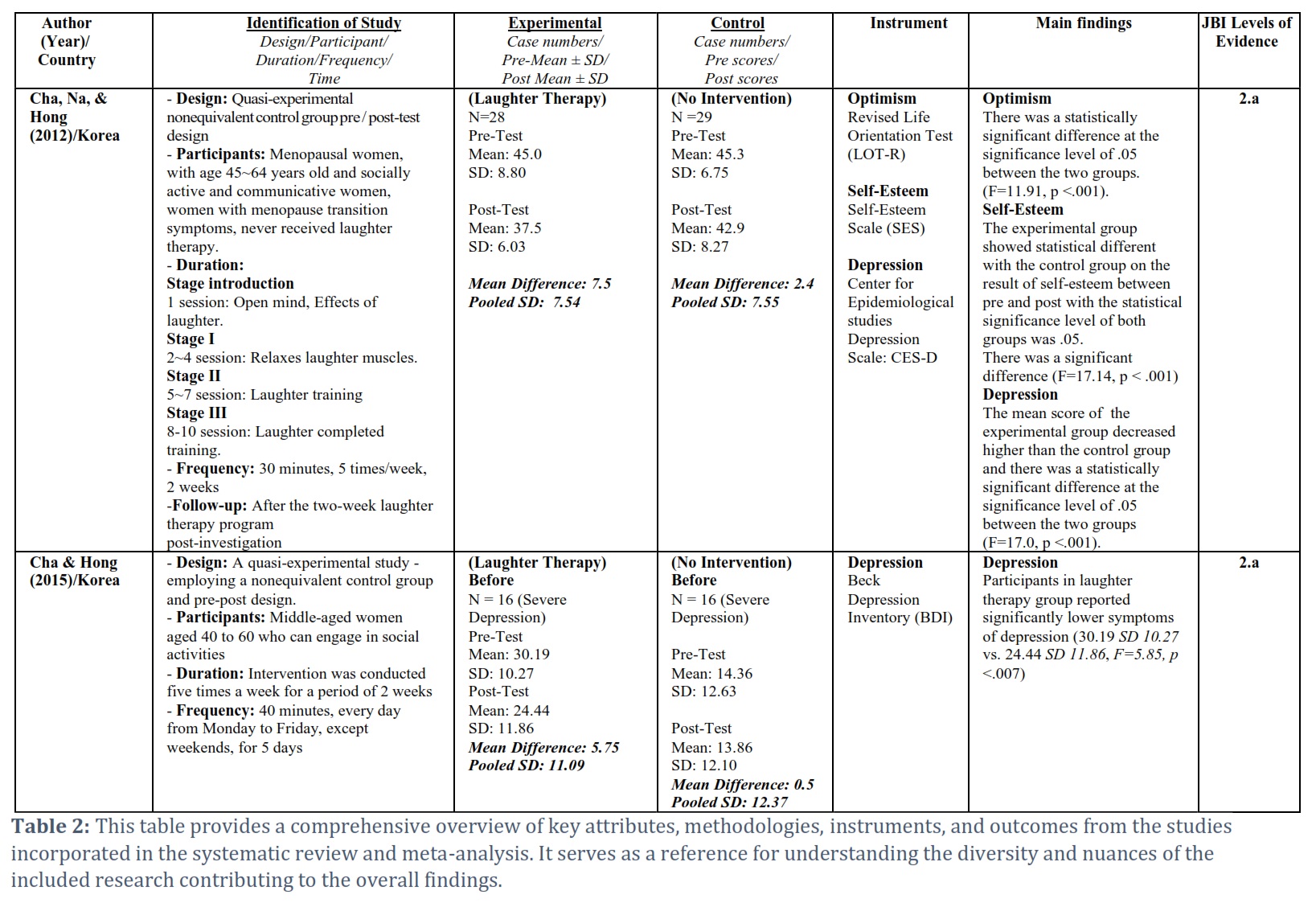
The two articles in the systematic review were quasi-experimental pre- and post-test designs, including the intervention and control groups. Studies originated in Korea and were conducted on 56 menopausal women aged 45–64 years old [19] and 32 middle-aged women with severe depression scores aged 40–60 years old [20]. The implemented intervention was similar in both articles, using laughter therapy for the intervention group and no intervention for the control group. The authors performed 10 sessions of laughter therapy, five times a week, for a total of two weeks. Laughter was induced through muscle relaxation and training. Before implementation, researchers conducted a pre-test of depression scores and re-evaluated them after the intervention, when the participants completed laughter training. The authors measured depression using the Center for Epidemiological Studies Depression Scale (CES-D) and Beck Depression Inventory (BDI) tools on menopausal women and middle-aged women, respectively. The details of the characteristics of inclusion studies are presented in Table 2.
Effect of Laughter Therapy on Depression among Middle-Aged Women
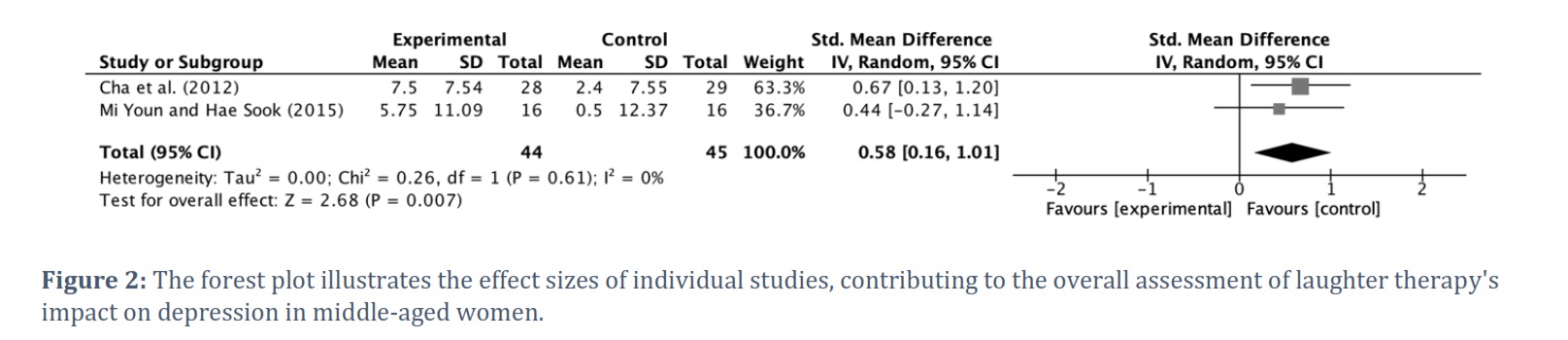
All Korean quasi-experimental studies demonstrated significant and beneficial results in reducing depression among 89 middle-aged women (SMD = .58, 95% CI (.16 to 1.01), p = 0.007) with a small to medium effect size pooled across studies. There was substantial evidence of high homogeneity in the studies (I2=0%) (Figure 2).
Figures & Tables

Laughter therapy is a form of communication that arouses laughter, smiles, and pleasant feelings and enables interaction. It utilizes laughter to treat and promote living a worthwhile life by keeping, recovering, and preventing physical, psychological, social, mental, and spiritual functions through different kinds of laughter [16]. On the other hand, depression is a mood disorder that is marked by varying degrees of sadness, despair, and loneliness and that is typically accompanied by inactivity, guilt, loss of concentration, social withdrawal, sleep disturbances, and sometimes suicidal tendencies [21]. Laughter on its own helps people to tolerate stressful situations and, in the process, decreases depressive symptoms. To the best of our knowledge, this is the first systematic review and meta-analysis to investigate the effects of laughter therapy on middle-aged women. We found that laughter therapy does reduce depression in middle-aged women. Moreover, laughter therapy improves different kinds of relationships, both psychological and social, by making them healthy [22].
A quasi-experimental nonequivalent control group pre/post-test design was done in Korea involving menopausal women who were aged 45-64 years old, socially active, and communicative, who had menopause transition symptoms, and who had never received laughter therapy before [19]. In this study, a laughter therapy program was applied at different stages as an intervention. There was an introduction stage where the participants in the experimental group were taught the clinical theory of laughter therapy and its effects, alongside practicing effective laughter techniques to induce active participation. After that, there were 3 stages: I, II, and III, involving laughter muscle relaxation and open mind stage, laughter training, and training completion stage, respectively. Here they had 30 minutes, 5 times a week for 2 weeks and then there was a post-investigation. The experimental group had less depression than the control group, and there was a statistically significant difference at the significance level of 0.05 between the two groups (F=17.0, p <.001). The results indicate that laughter could help reduce depression. Furthermore, it is clear that laughter therapy gives better results when the participants have been properly trained before being told just to practice.
Another quasi-experimental study employing a nonequivalent control group and a pre-post design was conducted in Korea [20]. In this study, they included middle-aged women, aged 40 to 60, who could engage in social activities, and they put them on laughter therapy for five times a week for a period of two weeks, with each session lasting 40 minutes. The intervention was done every day from Monday to Friday, for five days a week. The study reported that participants in the laughter therapy group reported significantly fewer symptoms of depression.
Therefore, it can be concluded that laughter therapy decreases depression among middle-aged women. The findings in this review align with a study done in an elderly population, which similarly concluded that laughter therapy is a useful and cost-effective way of reducing depression. They discovered that the mean Geriatric Depression Score was significantly decreased in the laughter therapy group after the intervention (P= 0.027) [22].
The findings are also consistent with a study that was done to investigate the effects of laughter therapy on depression in breast cancer patients, which concluded that there was a significant decrease in the levels of depression in the experimental group compared to those in the control group (p < 0.01) [23].
In this systematic review, we employed quantitative measures in both of the articles that were finally included. We used mean differences and pooled standard deviations in both the control groups and experimental groups in order to note the exact effects of laughter therapy instead of just reporting statistical significance between groups. As a result, we were able to provide a meaningful context for clinically relevant information about laughter therapy. After looking closely at these two articles, we found that laughter therapy is very helpful to middle-aged women since depression is one of the leading psychological problems affecting women twice as often as men in midlife [6]. According to the analysis, the risk of bias was assessed and found to be low.
A meta-analysis was done using RevMan5 software for quasi-experimental and the I-square was 0%, symbolizing high homogeneity, meaning good results since an I-square of 0% means there is no heterogeneity observed, 25% low heterogeneity, 50% moderate heterogeneity, and 75% high heterogeneity [24]. The p-value was 0.007, meaning the results are statistically significant. Therefore, we can conclude that laughter therapy does decrease depression among middle-aged women. After all the analysis, we found those on laughter therapy had significantly reduced depression. The aim of a meta-analysis was to use statistical approaches to derive a pooled estimate that is closest to the unknown common truth based on how this error is perceived [25]. For the Korean study [20], the mean difference was 5.75 and the pooled SD: was 11.09 for the experimental group, while for the control group, the mean difference was 0.5 and the pooled SD: was 12.37. On the other hand, the results of the meta-analysis for another Korean study [19] show a mean difference of 7.5 (pooled SD: 7.54) and a mean difference of 2.4 (pooled SD: 7.55) for the control group.
Quality assessment for quasi-experimental studies was done using ROBINS. Overall, both studies had a low risk of bias. Basically, the year 2012 Korean study [19] had a low risk of bias in all domains of the ROBINS, including bias due to confounding, bias in the selection of participants, bias in classifications, bias due to intended interventions, bias in measurements of outcomes, bias due to missing data, and bias in the selection of reported results. The other article, however, had a moderate risk of bias in three domains: bias due to confounding, bias due to participant selections, and bias due to missing data [20]. This is due to the fact that in this article, the authors had difficulties controlling confounding factors and there was no randomization done. Moreover, some participants dropped out, so there could be potential for missing data.
Critical appraisal for both articles was done using the JBI Critical Appraisal checklist for Quasi-Experimental Studies, tools for use in JBI Systematic Reviews. While the [19] article had “yes” answers on all 9 domains of the appraisal tool and was later included in our selection, the [20] article had a “no” in one domain, i.e., the participants included in the comparisons were not similar and the article made it clear that the assumption of normality was violated when tested with Kolmogorov-Smirnov’s normality test [20].
Limitations
This meta-analysis has several limitations. First, only 4 databases were searched (CINAHL, MEDLINE, Cochrane Library, and EMBASE), and possibly other psychological field studies were missed. Second, studies were limited to those published in Korean journals, and had a small sample size. Third, studies included in this meta-analysis were only conducted on Asian populations, which may limit the global generalizability of the results. Moreover, it could be hard to generalize the findings since the studies had small sample sizes of 32 and 57 participants. Ultimately, the absence of English-language articles posed a challenge in this systematic review. Both studies incorporated in the analysis were originally in Korean, necessitating translation through Google Translate and subsequent validation by a native Korean colleague. This process introduces the potential for language bias.
Practical implications
Laughter therapy could be a good strategy to reduce depression in middle-aged women as a non-pharmacological intervention. However, there is not enough evidence to support this recommendation, especially in clinical settings. Findings from this study are also in line with findings from another systematic review that was done on laughter-inducing therapies in 2019 [26]. The previous systematic review also suggested that laughter therapies are acceptable in different settings and for a broad range of patient groups. Although the results from these two included studies indicated a significant reduction in depression among middle-aged women, it is not sufficient to assert that this is a definitive treatment for depression. Depressed people still require medical and professional attention. Also, laughter therapy alone cannot be recommended as a sole treatment for depression since depression may need a mixture of treatments. In most cases, attention should be paid to the cause of depression instead of just depression itself.
Conclusion
The aim of this study was to examine the effectiveness of laughter therapy on depression outcomes in middle-aged women. The results show that laughter therapy has positive effects on depression status outcomes in middle-aged women. Laughter therapy appears to have a positive effect on optimism, self-esteem, depression, quality of life (QOL), and serotonin levels in middle-aged women. It has also been determined that laughter therapy provides a significant decrease in depression and serotonin levels. No research has documented any unfavorable outcomes of laughter therapy in middle-aged women. However, instances of laughter-induced syncope have been reported [27,28]. Although there are almost no contraindications, caution is suggested in patients who have recently undergone surgery, certain cardiovascular or respiratory conditions, or glaucoma [18]. Laughter therapy can be used for health promotion with the psychological in middle-aged women. It is a cost-effective and enjoyable technique for middle-aged women. In particular, in this meta-analysis, it has been found that the intervention duration required to affect the outcomes of middle-aged women appears to be at least 2 weeks, with a minimum of 30 minutes per session.
This meta-analysis suggests that laughter therapy can have beneficial effects on depressive outcomes in middle-aged women. According to the depression measures, the Center for Epidemiological Studies-Depression Scales (CES-D) and the Depression Inventory (BDI) were the clinical measures of depression. Cha et al., [19] used the self-report of the CES-D. Self-reported measures, despite their usefulness, lack objective measurement. Cha et al., [20] used self-reported BDI and serotonin levels as laboratory data.
The meta-analysis suggests that the number of studies and quality of data in this field are limited. In the future, it’s recommended for additional higher-quality RCTs to be designed with validated studies.
Author Contributions
Shannastaniar Aisya Adif: conceptualization, data analysis, data interpretation, data visualization, original draft preparation.
Muhammad Abdullah: conceptualization, data analysis, data interpretation, data visualization, original draft preparation.
Shih-Hsien Lin: data analysis, data interpretation, data visualization.
Huan-Fang Lee: supervision, manuscript editing.
The authors declare that there is no conflict of interest regarding the publication of this paper.
![]() References
References
- Abdullah M, Khan MI, Mumtaz F, Shah F, Ximenes RC, Nikoui V, et al. Risk factors associated with relapse of drug dependence after treatment and rehabilitation in areas under the influence of war on terror. Advancements in Life Sciences, (2020); 7(3) :117–121.
- Mimura M. Comorbidity of depression and other diseases. Japan Medical Association Journal. (2001); 5(44): 225–229.
- World Health Organization. (2021). Depressive disorder (depression) [Internet]. https://www.who.int/news-room/fact-sheets/detail/depression. [Accessed: 2022 October 23].
- Barry LC, Allore HG, Guo Z, Bruce ML, Gill TM. Higher burden of depression among older women: the effect of onset, persistence, and mortality over time. Archives of General Psychiatry, (2008); 65(2): 172–178.
- Barth C, Villringer A, Sacher J. Sex hormones affect neurotransmitters and shape the adult female brain during hormonal transition periods. Frontiers in Neuroscience, (2015); 9(37): 1-20.
- Sassarini DJ. Depression in midlife women. Maturitas, (2016); 94: 149–154.
- Prakapenka AV, Bimonte-Nelson HA. Memory and menopause: an unsolved puzzle. Aging, (2018); 10(10): 2541–2543.
- Bromberger JT, Epperson CN. Depression during and after the perimenopause: Impact of hormones, genetics, and environmental determinants of disease. Obstetrics and Gynecology Clinics of North America., (2018); 45(4): 663–678.
- Llaneza P, García-Portilla MP, Llaneza-Suárez D, Armott B, Pérez-López FR. Depressive disorders and the menopause transition. Maturitas, (2012); 71(2): 120–130.
- Dennerstein L, Soares CN. The unique challenges of managing depression in mid-life women. World Psychiatry, (2008); 7(3): 137–142.
- Karanth L, Chuni N, Nair NS. Antidepressants for menopausal symptoms. Cochrane Database of Systematic Reviews, (2019); (9): CD013417.
- Sim K, Lau WK, Sim J, Sum MY, Baldessarini RJ. Prevention of relapse and recurrence in adults with major depressive disorder: Systematic review and meta-analyses of controlled trials. International Journal of Neuropsychopharmacology, (2015); 19(2): pyv076.
- Craft LL, Perna FM. The benefits of exercise for the clinically depressed. Primary Care Companion to the Journal of Clinical Psychiatry, (2004); 6(3): 104–111.
- Brunoni AR, Sampaio-Junior B, Moffa AH, Aparício LV, Gordon P, Klein I, et al. Noninvasive brain stimulation in psychiatric disorders: a primer. Brazilian Journal of Psychiatry, (2019); 41(1): 70–81.
- Ekong MB, Iniodu CF. Nutritional therapy can reduce the burden of depression management in low income countries: A review. IBRO Neuroscience Reports, (2021); 11: 15–28.
- Yim J. Therapeutic benefits of laughter in mental health: A theoretical review. The Tohoku Journal of Experimental Medicine, (2016); 239(3): 243–249.
- Newland JA. Laughter is the best medicine. The Nurse Practitioner, (2020); 45(7): 6.
- Mora-Ripoll R. The therapeutic value of laughter in medicine. Alternative Therapies in Health and Medicine, (2010);16(6): 56–64.
- Cha MY, Na YK, Hong HS. An effect of optimism, self-esteem and depression on laughter therapy of menopausal women. Korean Journal of Women Health Nursing, (2012); 18(4): 248–256.
- Cha MY, Hong HS. Effect and path analysis of laughter therapy on serotonin, depression and quality of life in middle-aged women. Journal of Korean Academy of Nursing, (2015); 45(2): 221–230.
- Merriam-webster. Definition of DEPRESSION [Internet]. https://www.merriam-webster.com/dictionary/depression. [Accessed: 2022 October 23].
- Ko HJ, Youn CH. Effects of laughter therapy on depression, cognition and sleep among the community-dwelling elderly. Geriatrics and Gerontology International, (2011); 11(3): 267–274.
- Kim SH, Kim YH, Kim HJ, Lee SH, Yu SO. The effect of laughter therapy on depression, anxiety, and stress in patients with breast cancer undergoing radiotherapy. Asian Oncology Nursing, (2009); 9(2): 155–162.
- Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. British Medical Journal, (2003); 327(7414):557–560.
- Huang R, Wang K, Hu J. Effect of probiotics on depression: A systematic review and meta-analysis of randomized controlled trials. Nutrients, (2016); 8(8): 483.
- van der Wal CN, Kok RN. Laughter-inducing therapies: Systematic review and meta-analysis. Social Science and Medicine, (2019); 232: 473–488.
- Amaki M, Kamide K, Takiuchi S, Niizuma S, Horio T, Kawano Y. A case of neurally mediated syncope induced by laughter successfully treated with combination of propranolol and midodrine. International Heart Journal, (2007); 48(1): 123–127.
- Braga SS, Manni R, Pedretti RFE. Laughter-induced syncope. The Lancet, (2005); 366(9483): 426.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0