

Full Length Research Article
Changes of Serum Midkine as a Dynamic Prognostic Factor in Detection for Thyroid Cancer and Comparison with Fine-Needle Aspiration
Hadel Kareem Al-Rubaiawi¹*, Raid J. Mohamed2, Sajid H. Alhelfy3, Marwah S. Yones4
Adv. life sci., vol. 11, no. 2, pp. 425-429, May 2024
*– Corresponding Author: Hadel Kareem Al-Rubaiawi (Hadel_kareem@yahoo.com)
Authors' Affiliations
2. Department of Chemistry and Biochemistry, College of Medicine, Al-Nahrain University – Iraq
3. Department of surgery, College of Medicine, Al-Nahrain University – Iraq
4. Clinical Laboratory Science Branch, College of Pharmacy, Mustansiriyah University – Iraq
[Date Received: 24/12/2023; Date Revised: 06/02/2024; Date Available Online: 18/04/2024]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Midkine plays a significant role in the pathophysiology of malignant and other diseases since it is involved in a number of physiological processes, including development, reproduction, and repair. Different types of cells express this protein. Thus, in healthy conditions, significant MDK expression is observed in lymphocytes, the epidermis, and the bronchial epithelium. The sample obtained during fine needle aspiration can help in the diagnosis of or rule out disorders like cancer. Blood is the most practical and least likely bodily fluid to pollute while diagnosing illnesses. Finding successful prognostic markers in patients with well-defined thyroid cancer was the goal of the current investigation.
Methods: Midkine level was measured in serum samples by using Elisa technique for 80 patients (40 patient was diagnosed with papillary thyroid carcinoma and another 40 with benign thyroid goiter), Age (25-55) from Iraqis people.
Results: The current study revealed highly significant difference the median serum level of medkine in the TC patients was much higher than that of BTT patients with a highly significant difference The sensitivity and specificity of the test at cut off value of medkine=129 pg/ml were 90% for both. While FNA result, the sensitivity and specificity of FNAC was 80.77% and 89.66% respectively.
Conclusions: The thyroid cancer group's serum MDK result was noticeably higher than that of the healthy control groups. proposed that the midkine might serve as a biochemical marker for thyroid cancer early identification and diagnosis.
Keywords: Thyroid cancer; Papillary thyroid carcinoma; Midkine; ELISA; FNA
Introduction![]()
The most prevalent kind of endocrine cancer is thyroid cancer [1]. With a fairly excellent prognosis and minimal malignant potential, differentiated thyroid tumours (DTC) account for about 90% of thyroid neoplasms [2]. Thyroid cancer has become much more common within the past few decades.
According to estimates, thyroid cancer ranks ninth in terms of incidence in men and second in terms of frequency in women. It is currently the fifth most common cancer diagnosis in women. [3] The majority of thyroid cancers are caused by differentiated thyroid cancer (DTC), which mostly consists of follicular thyroid cancer (FTC) and papillary thyroid cancer (PTC).
Since early disease detection has been made possible by the aggressive use of US-guided fine needle aspiration biopsy (FNA) and more intense imaging with neck ultrasonography (US), there is a perceived higher incidence of DTC [4]. The initial course of treatment for most people with DTC involves a complete thyroidectomy. Nonetheless, patients with microcarcinomas who do not show nodal metastases on imaging may still undergo lobectomies [5].
Ultrasonography is the primary means of limited diagnostic technique, and percutaneous fine needle aspiration (FNA) is the gold standard for identifying benign and malignant thyroid nodules. These techniques, however, have a limited accuracy [6].
One of the first procedures in the surgical assessment of a thyroid nodule should be FNAC. Due in great part to sampling from cystic, haemorrhagic, hypervascular, or hypocellular colloid nodules, 15% of all aspirates are insufficient or nondiagnostic [7]. It is important to aspirate a nodule like this again since a nondiagnostic finding should never be used to rule out cancer. In 4% of women and 29% of men, surgical diagnosis following several nondiagnostic aspirations showed malignant nodules [8]. One kind of biopsy technique is fine needle aspiration. A tiny needle is introduced into a region of tissue or bodily fluid that appears abnormally in fine needle aspiration. The sample taken during fine needle aspiration, like with other biopsies, can aid in the diagnosis or ruling out diseases like cancer [9].
Alternative methods are required for precise detection potential blood markers for thyroid cancer. The most practical and difficult-to-contaminate bodily fluid for diagnosing conditions like midkine is blood.
The basic heparin binding growth factor with a low molecular weight, midkine, is related to pleiotrophin (NEGF1, 46% homologous with MK). The protein in question is non glycosylated and consists of two domains connected by disulfide bridges. Midkine is the name of a developmentally significant retinoic acid-responsive gene product that is substantially activated during mid-gestation. Mainly limited to certain tissues in the typical adult, it is highly activated during the processes of oncogenesis, inflammation, and tissue restoration. Because of its pleiotropic properties, MK can affect angiogenesis, fibrinolysis, cell migration, and proliferation [10].
Methods![]()
Study subjects
The study included 80 patients (female) with Goiter have a standard error of mean age (mean ± SE) 46.562 ± 1.105 years, Sample collected from patient before surgery . The Blood samples collection and the practical work of this study extended through twelve months from January 2022 until January 2023. Serum was collected from Al-Imameen Al-Kadohimin Teaching Hospital and Medicine City Hospital in Baghdad.
Patients were followed up after the operation to document the result of tissue histology examination. The patients were divided into Two groups. Group(1) include 40 sample serum of patient with benign thyroid goiter and another group(2) include 40 sample serum of patient diagnosed with thyroid cancer.
Measurement level of midkine level in serum
Enzyme-linked immunosorbent assay (ELISA) kits are used to assess the level of metabolites.
Statistical analysis
using SPSS version Analysis of variance will be used to compare means between the different groups and person’s correlation will be used to find midkine level in benign and malignant patient serum..
Results![]()
The median serum level of medkine in TC patients was 738 pg/ml (range= 118-1200 pg/ml) compared to 76 pg/ml (range= 36.71-233 pg/ml) in BTT patients with a highly significant difference, (figure 1).
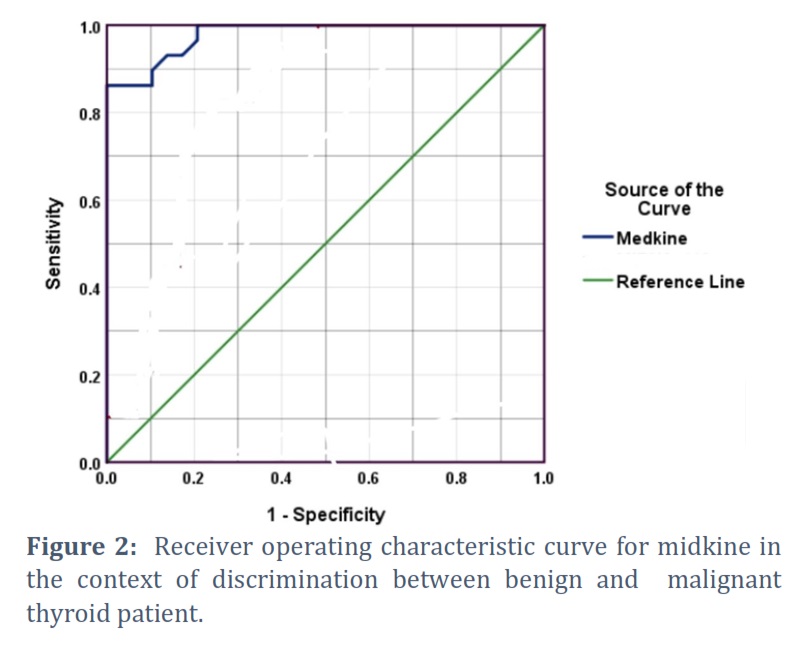
As these biomarkers showed significant variation between TC and BTT, they are candidates to be used for differentiation between the two conditions. Receiver operating curve (ROC) was used to find out the diagnostic value of these biomarker curve for medkine of discrimination between benign and malignant thyroid tumours the AUC was 0.979, 95%CI=0.951-1.00, p<0.001. The sensitivity and specificity of this marker test at cut off value of medkine= 129 pg/ml were 90% for both as shown in figure 2.
The FNAC was available for 26 patients with TC and 29 patients with BTT. Out of 26 patients with TC, 21 patients (80.77%) were positive for FNAC as true TC. On the other hand, out of 29 patients with BTT, 3 patients (10.34%) had a positive FNAC as shown in (Figure 3).
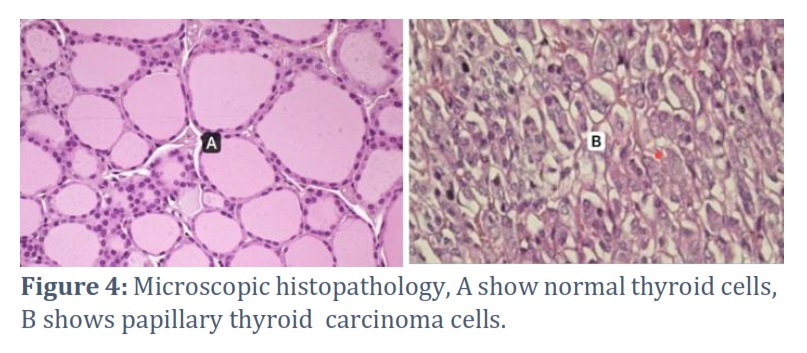
Out of 26 TC patients according to histopathological examination, 21 were also positive for FNAC. On the other hand, 26 patients out of 29 patients with BTT based histopathology were also found to be negative for FNAC. Accordingly, the sensitivity and specificity of FNAC was 80.77% and 89.66% respectively. Figure 4 shows the microscopic histopathology of papillary thyroid carcinoma in FNA sample.
Figures & Tables
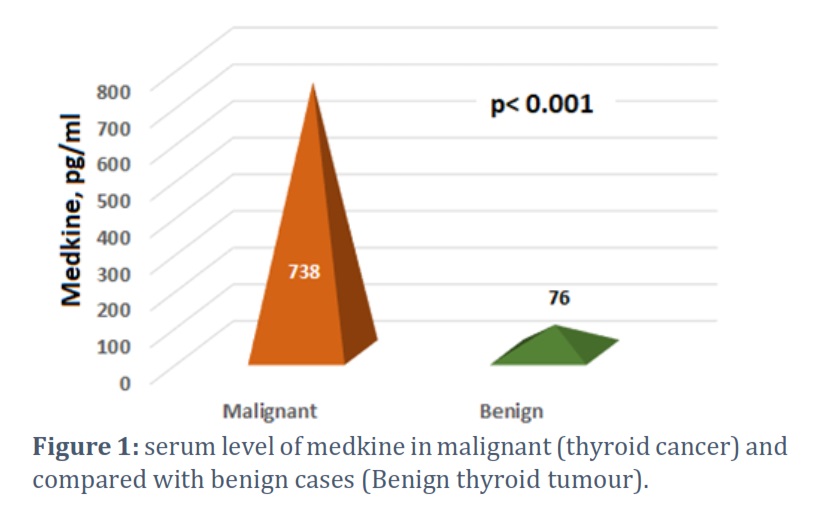

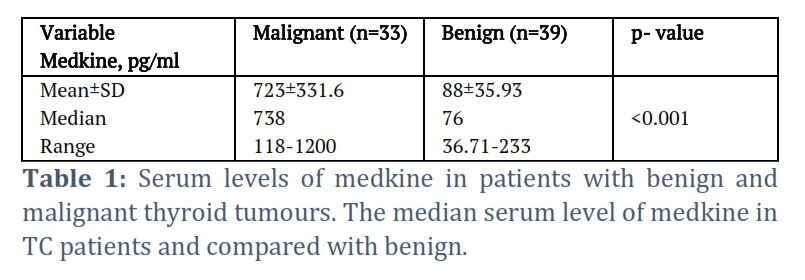
In the present study the median serum level of medkine in TC patients was 738 pg/ml (range= 118-1200 pg/ml) which much higher than that of BTT patients (median= 76 pg/ml, range= 36.71-233 pg/ml) with a highly significant difference. the AUC was 0.979, 95%CI=0.951-1.00, p<0.001. A prior study was carried out by Mahmoud et al., [10]. The Elisa Technique was used to quantify midkine in patients with thyroid cancer compared to patients with benign thyroid disorders. In this study, there 29 patients with benign thyroid illness, and 27 patients with thyroid cancer. Elevated level of medkine in patient with thyroid cancer, Individuals diagnosed with stage III thyroid cancer had elevated levels of midkine relative to those diagnosed with stages I and II (p < 0.001). Compared to patients with grade I, patients with grade II had greater midkine (p < 0.001). When thyroid carcinoma was detected using ROC analysis, midkine had an AUC of 0.95 at a threshold of 897.5 pg/ml, 98.0% sensitivity, and 81.5% specificity (p < 0.001).
In another investigation, fifteen healthy controls with age- and sex-matched thyroid cancer cases were compared to patients with benign thyroid problems by Abdel-Azeem et al., [11]. ELISA was used to measure the level of serum midkine. Thyroid cancer patients had far higher levels of midkine than both the control group and those with benign thyroid diseases. Midkine was reported to have an accuracy of 88.4%, a specificity of 98.18%, sensitivity of 83.3%, and an area under the curve of 0.95 at the cutoff point of 895 pg/ml. They came to the conclusion that the serum midkine level, which correlates with tumour stage, is a useful diagnostic for thyroid cancer screening.
A further study from Iraq's University of Kufa in Najaf by Gebur et al., [12]. In a case-control study, 120 Iraqi participants—60 of them female and 12 of them male—had thyroid cancer. The results were compared to those of 60 healthy adults—50 of whom were female and 10 of whom were male—whose ages were similar to those of the patient group, which ranged from 27 to 60 years. The thyroid cancer group’s serum MDK result was considerably higher (202.1 ± 47.4 versus 149.6 ± 41.0 ng/mL, P=0.003) than the healthy control groups, shown that midkine might function as a biochemical marker for thyroid cancer early identification and diagnosis. This study confirms the findings of every other study stated, showing that TC patients had significantly greater serum levels of medkine than BTT patients did. Additionally, it was suggested that midkine might function as a biochemical marker for thyroid cancer early identification and detection. Some variations in the number of samples and the patient’s environment can lead to varied outcomes. Pre-operative diagnostic tests such as fine needle aspirations (FNA), CT scans, and ultrasounds can yield conflicting results [13]. Therefore, biomarkers are necessary for diagnosis. Midkine (MK) is a pleiotropic growth factor that is extensively expressed throughout the embryonic stage. It regulates cell migration, proliferation, and survival as well as angiogenic and anti-apoptotic processes [14]. Given that MK is a soluble cytokine that is widely distributed in the bloodstream, tumor cancer cells have more permeability, which may allow proteins that originated from the tumor to pass through by increasing cell permeability to serum, so Midkine was released into the blood from cancerous tissue [15]. Its advantage is that it’s a non-invasive, reasonably useful biomarker [16].
Thyroid cancer is one of the types of cancers that cannot be diagnosed with a thyroid marker in blood before the operation, Relying mainly on FNA.
So, in this study was evaluating the midkine level in serum, this provides a diagnostic tool to differentiate the benign thyroid tumour form thyroid cancer. It may also serve as the novel therapeutic target for thyroid cancer.
Ethical Clearance
The Iraqi scientific research committee for ethics in research has the consent of the ministries of higher education, health, and the environment.
Conflict of Interest
The authors declare that there is no conflict of interest.
Hadel Kareem. AL-Rubaiawi : Drafting the article, designing the experiment, summarizing the results, and proposing the research paper.
Raid J. Mohamed: Preparing materials, Funding acquisition, Data curation, Statistical analysis and review & editing
Sajid H. Alhelfy: Collecting sample , the sample collected during fine needle aspiration to make a diagnosis.
![]() References
References
- Omur O, Baran Y. An update on molecular biology of thyroid cancers. Critical reviews in oncology hematology, (2014); 90(3):233-252.
- Rivkees SA, Mazzaferri EL, Verburg FA, Reiners C, Luster M, Breuer CK, Dinauer CA, Udelsman R.. The treatment of differentiated thyroid cancer in children emphasis on surgical approach and radioactive iodine therapy. Endocrine reviews, (2011); 32(6): 798-826.
- Twining CL, Lupo MA, Tuttle RM. Implementing key changes in the American Thyroid Association 2015 thyroid nodules/differentiated thyroid cancer guidelines across practice types. Endocrine Practice, (2018); 24(9):833-840.
- Diamantis A, Magiorkinis E, Koutselini H. Fine-needle aspiration (FNA) biopsy historical aspects. Folia histochemica et cytobiologica, (2009); 47(2):191-197.
- Lee J, Park JH, Lee CR, Chung WY, Park CS. Long-term outcomes of total thyroidectomy versus thyroid lobectomy for papillary thyroid microcarcinoma comparative analysis after propensity score matching. Thyroid, (2013); 23 (11) :1408-1415.
- Hong AR, Lim JA, Kim TH, Choi HS, Yoo WS, Min HS, Won JK, Lee KE, Jung KC, Park DJ, Park YJ. The frequency and clinical implications of the BRAFV600E mutation in papillary thyroid cancer patients in Korea over the past two decades. Endocrinology and Metabolism, (2014); 29 (4):505-513.
- Harkin C, Cobice D, Brockbank S, Bolton S, Johnston F, Strzelecka A, Watt J, Kurth MJ, Lamont JV, Fitzgerald P, Moore T. Biomarkers for detecting kidney dysfunction in type-2 diabetics and diabetic nephropathy subjects a case-control study to identify potential biomarkers of DN to stratify risk of progression in T2D patients. Frontiers in Endocrinology, (2022); 13:887237.
- Gupta MK, Qin RY. Mechanism and its regulation of tumor-induced angiogenesis. World journal of gastroenterology, (2003); 9(6):1144.
- Kim SW, Lee JI, Kim JW, Ki CS, Oh YL, Choi YL, Shin JH, Kim HK, Jang HW, Chung JH. BRAF V600E mutation analysis in fine-needle aspiration cytology specimens for evaluation of thyroid nodule a large series in a BRAF V600E-prevalent population. The Journal of Clinical Endocrinology & Metabolism, (2010); 95(8): 3693-3700.
- Mahmoud AA, Mohamed HO, AM AA, Abdelghafour HS, Jabir MA. Long noncoding RNA HOTAIR and Midkine as biomarkers in thyroid cancer. The Egyptian Journal of Immunology, (2023); 30 (1):96-104.
- Abdel-Azeem HG, Abdel-aal AM, Mahran MH, Thabet MH. The Role of Serum Midkine and Secretory Leucocyte Protease Inhibitor in Diagnosis of Thyroid Cancer. The Egyptian Journal of Hospital Medicine, (2022); 89(1):6039-5.
- Gebur NA, Ali HA. Association between Levels of Serum Midkine with Insulin Resistance as New Potential Diagnostic Marker for Thyroid Cancer in its Early Stages. Clinical Schizophrenia & Related Psychoses, (2021);15.
- Wiseman SM, Baliski C, Irvine R, Anderson D, Wilkins G, Filipenko D, Zhang H, Bugis S. Hemithyroidectomy the optimal initial surgical approach for individuals undergoing surgery for a cytological diagnosis of follicular neoplasm. Annals of surgical oncology, (2006); 13:425-432.
- Muramatsu T, Kadomatsu K. Midkine an emerging target of drug development for treatment of multiple diseases. British journal of pharmacology, (2014); 171(4):811-813.
- AL-Rubaiawi HK, Mohamed RJ. The Activity of 5-Flurouracil Metabolizing Enzyme Dihydropyrimidine Dehydrogenase (DPD) and its Association with Tumor Progression and Markers (CEA, CA19. 9) in Patients with Colorectal Cancer. Indian Journal of Public Health Research & Development,(2019); 10(10):1
- Jones D R. Measuring midkine: the utility of midkine as a biomarker in cancer and other diseases. British journal of pharmacology, (2014);171(12): 2925-2939.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0