

Full Length Research Article
Severity Assessment and IL-5 Evaluation after Immunotherapy in Atopic Dermatitis Mice
Sylvia Anggraeni1,2, Dinar Chieko Triesayuningtyas2, Hamidah Luthfidyaningrum2, Made Putri Hendaria2, Yuri Widia2, Anang Endaryanto3, Cita Rosita Sigit Prakoeswa2
Adv. life sci., vol. 11, no. 2, pp. 309-314, May 2024
*– Corresponding Author: Cita Rosita Sigit Prakoeswa (cita-rosita@fk.unair.ac.id)
Authors' Affiliations
2. Department of Dermatology and Venereology, Faculty of Medicine Universitas Airlangga/Dr. Soetomo General Academic Hospital, Surabaya – Indonesia
3. Department of Pediatrics, Faculty of Medicine Universitas Airlangga/Dr. Soetomo General Academic Hospital, Surabaya – Indonesia
[Date Received: 29/12/2022; Date Revised: 27/08/2023; Date Available Online: 18/04/2024]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: The effectiveness of immunotherapy in atopic dermatitis (AD) has been debated for many years. Immunotherapy suppresses Th2 cytokines, such as IL-5, which play a crucial role in the pathogenesis of AD. This study assessed the effect of immunotherapy on severity and IL-5 expression in AD mice.
Methods: Male BALB/c mice were separated into three groups. The mice were sensitized with Dermatophagoides pteronyssinus allergen for seven days, except the mice in control group. The house dust mite (HDM) immunotherapy was injected subcutaneously every 3 days for 1.5 months with increasing doses (0.1, 1, 10, 100 μg in 100 μL PBS) every 4 injections. The mice in AD model and control group received placebo injections. Following immunotherapy, the mice were exposed to HDM allergen patch two times with 2 weeks interval in between. The mice were evaluated for severity score as the clinical marker and IL-5 expression with semiquantitative method as the histological marker.
Results: The evaluation of severity score from two independent researchers showed a substantial agreement (Cohen’s kappa 0.613, p <0.001). The severity score of the immunotherapy group was significantly lower than the AD model group, while both immunotherapy and AD model group had significantly higher score than control group. IL-5 expression in the immunotherapy group was lower than the AD model group and slightly higher than control group. The mean difference between groups was not significant.
Conclusion: The severity of skin lesion and IL-5 expression in AD mice receiving immunotherapy were lower than AD model group.
Keywords: Atopic dermatitis; BALB/c mice; House dust mites; IL-5, Skin severity score; Tropical disease
Introduction![]()
Atopic dermatitis (AD) can cause lifestyle changes, impaired social interaction, limitations in activities, sleep disturbances, anxiety, low self-confidence, and depression. Chronic diseases not only cause a decrease in the quality of life, but high medical expenses are also an important issue. Atopic dermatitis is a chronic skin disease that often causes an economic burden [1–3]. There is a rise in the number of AD cases worldwide, including in Surabaya, Indonesia, where AD cases are mainly found in boys (53.4%) and age range of 5-14 years old (46.6%) [4].
Good hygiene, use of antibiotics, and vaccinations cause the body to be less exposed to microorganisms and cause a shift in the immune reaction towards allergic diseases. Air pollution is also one of the triggering factors for AD [3]. The most common environmental factor is house dust mites (HDMs). Dermatophagoides pteronyssinus and Dermatophagoides farinae are the two mite species that are most frequently seen in Indonesia. According to a study, 57.77% of people with AD were sensitized to HDM, as indicated by positive skin prick test results using a local Dermatophagoides pteronyssinus allergen extract [5]. Similar to allergic rhinitis and asthma, HDM allergens can trigger a type 2 immune response and the production of interleukin (IL)-4, IL-5, and IL-13 [6].
Allergen sensitization through the respiratory tract generally causes allergic rhinitis and asthma, whereas exposure through the skin will trigger AD. Immune dysregulation is a concept that has long been associated with atopic dermatitis. Th2 cytokines (IL-4, IL-5, IL-13, and IL-31) are released by Langerhans Cells (LC) and Inflammatory Dendritic Epidermal Cells (IDEC) in response to damage to the epidermal barrier caused by genetic and environmental factors. This condition also triggers Thymus and Activation Regulated Cytokines (TARC), ILC-2 is activated by thymic stromal lymphopoietin (TSLP), IL-25, and IL-33, which promotes the synthesis of IL-5 and IL-13 [7,8].
Although progress has been made in the treatment of AD, there is currently no satisfactory treatment for the disease due to its chronic and recurring characteristic [9]. Immunotherapy can be recommended in atopic diseases such as rhinitis allergy and asthma [10]. Meanwhile, the Joint Task Force and The European Academy of Dermatology recommend that immunotherapy can only be given to severe AD, with exacerbation of exposure to aeroallergens, especially HDMs. There are no fixed immunologic biomarkers for predicting the effectiveness of immunotherapy, although some attempts had been made [11]. Immunotherapy suppresses cytokine axis. Th2 cells produce cytokines, including IL-3, IL-4, IL-5, IL-9, and IL-13, which play a crucial role in the survival, activation, and differentiation of mast cells, basophils, and eosinophils in AD [12]. This study assessed the severity score and IL-5, one of the main cytokines in AD, as an immunological marker of specific immunotherapy in AD mouse model.
Methods![]()
This was an experimental study which involved male BALB/c mice, 6-8 weeks old. Thirty-three mice were bought from Faculty of Veterinary Medicine Universitas Airlangga and randomly assigned to groups namely (1) immunotherapy group, (2) AD model group, and (3) control group. The mice were kept in individual cages made of plastic with 12 x 8 x 8 cm in size. Ad libitum food and water were provided to the mice.
Induction of AD-like lesion in mice
For the HDM sensitization phase, a patch containing HDM allergen or placebo was placed to the back of the mouse that had been shaved. The patch, a 1×1 sterile gauze, was put in place with a hypoallergenic tape. Allergen spray was done for 30 minutes per day for 7 days. The mice were allowed to familiarize themselves with the spray chamber made of plastic with 30 x 40 x 40 cm in size, for 1 hour prior to the treatment. The spray chamber was connected to a nebulizer where the allergen was diffused. The allergen used for sensitization was Dermatophagoides pteronyssinus with a dose of 100 ug for patch and 10-6 ug for spray. The control group was given normal saline for both patch and spray. The allergen spray was continued every day for 93 days, throughout the sensitization and immunotherapy until the end of the treatment.
Subcutaneous Immunotherapy
The immunotherapy started a week after the end of sensitization phase. The immunotherapy used Dermatophagoides pteronyssinus allergen in escalating doses of 0.1, 1, 10, and 100 μg in 100 ml phosphate-buffered saline (PBS). The allergen was developed by Dr. Soetomo Hospital's Teaching Industry Allergen from Universitas Airlangga in Surabaya, Indonesia [10]. The subcutaneous injection to the neck of the mouse was given every 3 days and the dose was increased after every 4 injections. Mice in the AD model and control group received placebo injections using PBS. The mice were exposed to HDM allergen patch two times in 2 weeks interval with the same protocol as the sensitization phase, after the immunotherapy had finished.
Evaluation of severity score
The mice's skin lesion on their backs was assessed for severity on day 93. The overall scores were calculated by adding the scores of the following symptoms: erythema/hemorrhage, edema, excoriation/erosion, and dryness. The score ranges from 0 to 3 (0, no symptoms; 1, mild; 2, moderate; 3, severe) and the overall score ranges from 0 to 12. The evaluation was done by two independent researchers and the agreement between the two was assessed with Cohen’s kappa analysis.
Immunohistochemical examination
The skin tissues from the backs of the mice were gathered and analyzed for IL-5 expression using immunohistochemistry (IHC) method. The skin tissues were embedded in paraffin, fixed with 10% paraformaldehyde, sectioned into 4 μm thick sections, and then stained with immunostaining. To assess the IL-5 expression, a semiquantitative immunoreactive score (IRS) scale was applied. The percentage of positive cells and the intensity of the color reaction were both measured, then the scores were multiplied to obtain the IRS (Table 1). The IRS from 10 fields of view were counted for the average score of each mouse.
Statistical analysis
The data were then analyzed using IBM's SPSS Software version 26 for both descriptive and comparative analysis. For data with a normal distribution, the One-Way ANOVA test was used; for data with a non-normal distribution, the Kruskal-Wallis test was used.
Ethical clearance
The ethical clearance for this study was issued by Faculty of Veterinary Medicine Universitas Airlangga (No. 2.KE.11.09.2021).
Results![]()
Severity score assessment
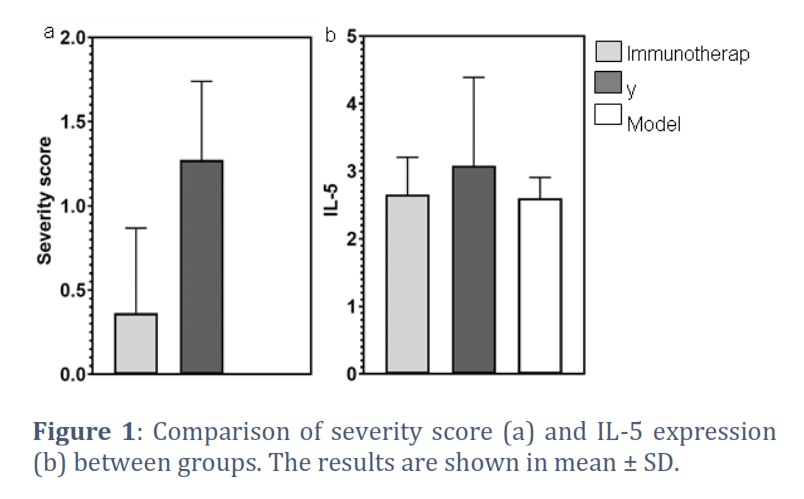
The evaluation of severity score from two independent researchers showed a substantial agreement (Cohen’s kappa 0.613, p <0.001). The severity score of the immunotherapy group was lower than the AD model group while the control group showed no skin lesion (Figure 1a). Statistical analysis using the Kruskal-Wallis test showed a significant difference between the groups. Further analyses with Mann Whitney test found that there were significant differences between immunotherapy and AD model group (p = 0.001), immunotherapy and control group (p = 0.031), as well as AD model and control group (p <0.001).
IL-5 assessment
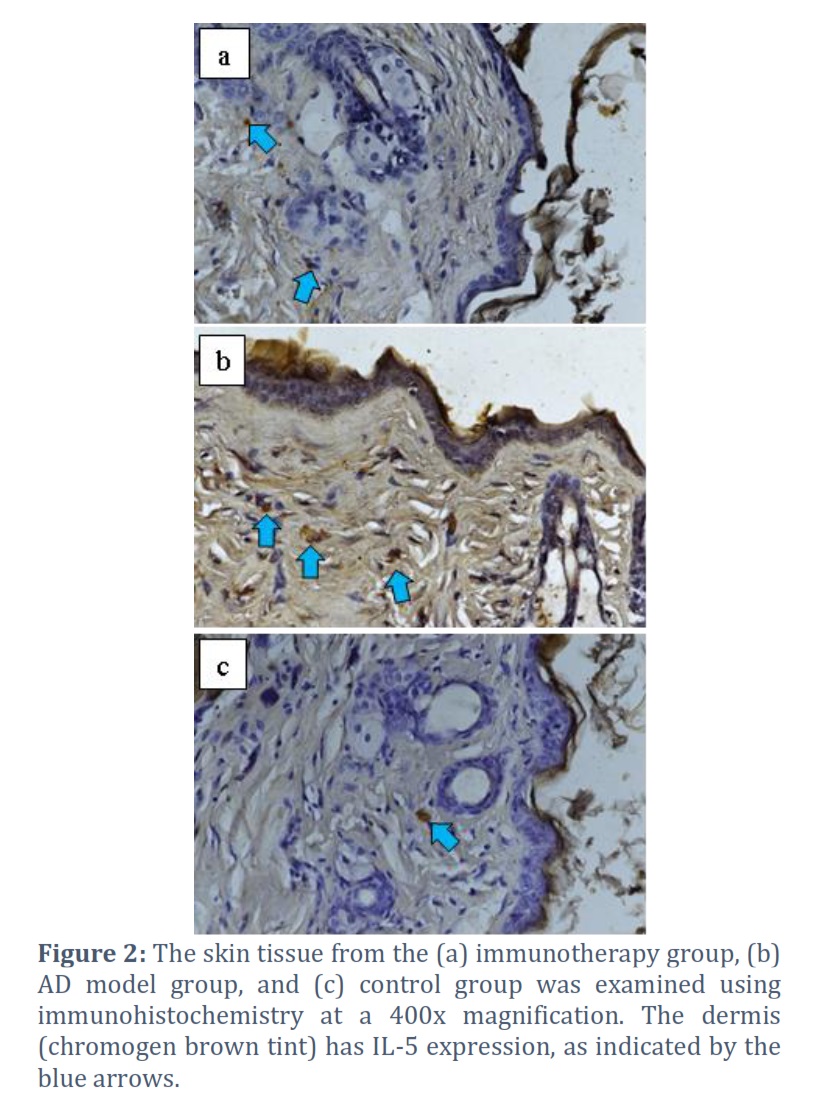
The mice were sacrificed on day 93 and IL-5 expression from the skin tissue was analyzed. The mice in immunotherapy showed lower mean ± SD of IL-5 expression compared to AD model group with 2.655 ± 0.552 and 3.082 ± 1.307, respectively. While the IL-5 expressions of immunotherapy and control group showed similar mean value with 2.6 ± 0.310 (Figure 1b). However, the comparative analysis using One Way ANOVA indicated that there was no significant difference between the groups (p = 0.349). The immunohistochemistry examination showed chromogen brown color of the IL-5 (Figure 2).
Figures & Tables

Atopic dermatitis is mainly a type 2 inflammatory disorder with the major cytokines and alarmins including IL-4, IL-5, IL-13, IL-31, IL-25, Thymic stromal lymphopoietin (TSLP), and IL-33. Type 2 inflammation is caused by damage to the skin barrier, and this in turn leads to more barrier damage. In acute AD, immune cell infiltration results in type 2-mediated release of inflammatory cytokines, while barrier disturbances in compromised skin promote permeability and penetration of pathogens or allergens. In acute eczematous lesions, epithelial barriers are disrupted and there are increased Langerhans cells with dendrites entering through tight junctions. Type 2 inflammatory responses (e.g., FLG, lipids, and AMPs) cause epithelial remodeling and proliferation, resulting in chronic lesions [14]. TSLP increases the production of OX40 ligand (OX40L) in dendritic cells and induces naïve CD4(+) T cells differentiation. The Th2 cytokines are produced by the differentiation of naïve CD4(+) T cells into Th2 cells [8]. IL-4 and IL-13 cytokines stimulate the Th2 response, whereas IL-3, IL-5, and Granulocyte-macrophage colony-stimulating factor (GM-CSF) cause the generation and activation of eosinophils [15]. Eosinophils have a significant role in type 2 immunity. In AD patients, serum eosinophils are elevated. Eosinophils can also be found in skin biopsies from both acute and chronic AD lesions [16].
House dust mites-derived airborne allergens can cause AD exacerbation. In individuals with AD, tight junctions are known to be disrupted by allergens and the skin barrier function deteriorates as a result of their enzymatic activity. Proteins from house dust mites can enter the epidermis through this disruption of the skin barrier, where they can then stimulate the type 2 inflammatory response and exacerbate AD [17]. Dermatophagoides pteronyssinus (Der p) is a prevalent HDM species with Der p 1 and Der p 2 as the primary allergens. The epitope vaccine derived from Der p 1 allergen was found to have a good hope to be developed as allergen specific immunotherapy in atopic diseases [18].
The use of immunotherapy in AD has now become the subject of further research. The results of several systematic reviews on immunotherapy in AD were inconclusive, and no clear recommendations could be provided. According to a meta-analysis, specific immunotherapy using a standardized aeroallergen extract can significantly lower the Scoring Atopic Dermatitis (SCORAD), Visual Analog Score (VAS) in AD patients [11,19]. Immunotherapy attempts to improve the patient’s tolerance to allergen exposure. Patients are desensitized by injection with increasing doses of allergen, beginning with small dose [15]. Successful SIT is thought to be mediated by the same cellular mechanisms that result in immune deviation with a shift in Th profile from Th2 to Th0/Th1, induction of Treg cells, a rise in IFNγ synthesis, or the development of natural immune tolerance in the absence of co-stimulation [20].
Th2-biased profiles in acute AD are thought to be the outcome of either enhanced differentiation of Th2 cells or greater activation and death of Th1 cells with high levels of IFNγ production. It is well recognized that these Th1 cells play a role in AD epithelial apoptosis. The induction of Treg cells during targeted immunotherapy facilitates the suppression of Th1 and Th2 cytokines and allergen-induced T-cell proliferation. Thus, clinical improvement in AD may be seen as a result of decreased skin inflammation and epithelial apoptosis [12]. The mice in immunotherapy group in this study were found to have milder skin lesion which was indicated by significantly lower severity score compared to the AD model group receiving placebo injections. A study of HDM immunotherapy in AD mouse model reported of similar results, but the difference between groups was not significant at the end of the treatment on week 8 [21].
Immunohistochemistry (IHC) is a basic method for identifying specific antigens in tissue which have diagnostic, differential diagnostic, and prognostic importance [22]. Pathologists’ subjective assessments of the expression of IHC markers can be converted into quantitative data using semiquantitative scoring methods. This data is then utilized for statistical studies and the establishment of conclusions [23]. Though board-certified pathologists are highly skilled at identifying patterns in histopathological changes the human visual system is not very good at picking up on tiny alterations in tissues, especially when it comes to spatial and intensity assessments [22]. Automated calculation of histopathological parameters that is more objective and less time-consuming can be very helpful but there haven’t been an ideal automated system available, and high costs as well as special skills to operate the system are likely to be required [23]. Immunoreactive scale (IRS) was used in this study as this semiquantitative method had been used in previous studies [13]. The subjectivity of this method can affect the calculation of the results which might be one of the limitations of this study. Therefore, the calculation of IRS in each sample was done in 10 fields of view and was counted for the average score. After receiving immunotherapy in escalating doses, the average score of IL-5 expression in the immunotherapy group was lower than the AD model group. This finding indicates that a shift in Th2 to Th0/Th1 after immunotherapy resulted in the decrease of Th2 cytokines including IL-5. A similar study utilizing ovalbumin allergen for immunotherapy in an AD mice model also found a decrease in spleen IL-5 expression compared to the group without immunotherapy. However, the results were not statistically significant [24].
The use of specific immunotherapy in AD has a good prospect and the mechanism of immunotherapy in this disease is still being investigated through many studies. Currently available research on specific immunotherapy effectiveness in AD demonstrate that it has a good clinical efficacy in treating individuals who are allergic to aeroallergens [20]. Finding a biomarker that can reliably predict therapy response is an important goal. Nevertheless, doing so is difficult given the complex and intricately intertwined immunologic processes and axis that are involved in atopic diseases [12]. IL-5 as one of the main cytokines in AD pathogenesis can describe one side of the immunotherapy effect on the disease.
In conclusion, the severity of skin lesion and IL-5 expression in AD mice receiving immunotherapy were lower than placebo group.
Funding
This research was supported by Faculty of Medicine, Universitas Airlangga, Surabaya, Indonesia.
Acknowledgement
We would like to thank Faculty of Medicine, Universitas Airlangga, Surabaya, Indonesia for supporting this research.
Conflict of Interest
The authors declare that there is no conflict of interest.
Conceptualization: Sylvia Anggraeni, Anang Endaryanto, Cita Rosita Sigit Prakoeswa
Data Curation: Sylvia Anggraeni, Dinar Chieko Triesayuningtyas, Anang Endaryanto
Formal Analysis: Sylvia Anggraeni, Dinar Chieko Triesayuningtyas, Anang Endaryanto
Funding Acquisition: Cita Rosita Sigit Prakoeswa
Investigation: Dinar Chieko Triesayuningtyas, Hamidah Luthfidyaningrum, Made Putri Hendaria, Yuri Widia
Methodology: Sylvia Anggraeni, Yuri Widia
Administration: Sylvia Anggraeni
Resources: Sylvia Anggraeni, Dinar Chieko Triesayuningtyas, Hamidah Luthfidyaningrum, Made Putri Hendaria, Yuri Widia
Software: Sylvia Anggraeni, Dinar Chieko Triesayuningtyas
Supervision: Anang Endaryanto, Cita Rosita Sigit Prakoeswa
Writing: Original Draft Preparation: Sylvia Anggraeni, Dinar Chieko Triesayuningtyas, Hamidah Luthfidyaningrum
Writing: Review & Editing: Hamidah Luthfidyaningrum, Made Putri Hendaria, Yuri Widia
![]() References
References
- Feldman SR, Cox LS, Strowd LC, Gerber RA, Faulkner S, et al. The challenge of managing atopic dermatitis in the United States. American Health & Drug Benefits, (2019); 12(2): 83.
- Silverberg JI, Gelfand JM, Margolis DJ, Boguniewicz M, Fonacier L, et al. Patient burden and quality of life in atopic dermatitis in US adults: A population-based cross-sectional study. Annals of Allergy, Asthma and Immunology, (2018); 121(3): 340–7.
- Urban K, Chu S, Giesey RL, Mehrmal S, Uppal P, et al. The global, regional, and national burden of atopic dermatitis in 195 countries and territories: an ecological study from the Global Burden of Disease Study 2017. JAAD International, (2021); 2: 12–8.
- Sihaloho K, Indramaya DM. Penelitian Retrospektif : Dermatitis Atopik pada Anak. Berkala Ilmu Kesehatan Kulit dan Kelamin, (2015); 27(3): 176–82.
- Anggraeni S, Umborowati MA, Damayanti, Endaryanto A, Rosita Sigit Prakoeswa C. Correlation between Skin Prick Test and Specific IgE of Local Mites Allergen in Atopic Dermatitis Patients: an Indonesian Study. Chiang Mai University Journal of Natural Sciences, (2022); 21(4): e2022053.
- Alvaro-Lozano M, Akdis CA, Akdis M, Alviani C, Angier E, et al. Allergen Immunotherapy in Children User’s Guide. Pediatric Allergy and Immunology, (2020); 31(Suppl.25): 1–101.
- Cho YT, Chu CY. Advances in systemic treatment for adults with moderate-to-severe atopic dermatitis. Dermatologica Sinica, (2019); 37(1): 3.
- Yang G, Seok JK, Kang HC, Cho YY, Lee HS, et al. Skin barrier abnormalities and immune dysfunction in atopic dermatitis. International Journal of Molecular Sciences, (2020); 21(8).
- Herwanto N, Hutomo M. Retrospective Study: Management of Atopic Dermatitis. Berkala Ilmu Kesehatan Kulit dan Kelamin, (2016); 28(1): 45–54.
- Putera AM, Hikmah Z, Endaryanto A, Irwanto, Maramis MM. The role of house dust mite immunotherapy in Indonesian children with chronic rhinosinusitis allergy: A randomized control trial. Heliyon, (2021); 7(3).
- Caminiti L, Panasiti I, Landi M, de Filippo M, Olcese R, et al. Allergen immunotherapy in atopic dermatitis: Light and shadow in children. Pediatric Allergy and Immunology, (2020); 31(Suppl.26): 46–8.
- Lee J, Park CO, Lee KH. Specific immunotherapy in atopic dermatitis. Allergy, Asthma & Immunology Research, (2015); 7(3): 221–9.
- Nowak M, Madej JA, Dzięgiel P. Intensity of COX2 Expression in Cells of Soft Tissue Fibrosarcomas in Dogs as Related to Grade of Tumour Malignancy. Bulletin of the Veterinary Institute in Pulawy, (2007); 51: 275–9.
- Beck LA, Cork MJ, Amagai M, de Benedetto A, Kabashima K, et al. Type 2 Inflammation Contributes to Skin Barrier Dysfunction in Atopic Dermatitis. JID Innovations, (2022); 2(5): 100131.
- Murphy K, Weaver C, Janeway C. Janeway’s immunobiology 9th edition. 2017; New York: Garland science.
- Hassoun D, Malard O, Barbarot S, Magnan A, Colas L. Type 2 immunity-driven diseases: Towards a multidisciplinary approach. Clinical and Experimental Allergy, (2021); 51(12): 1538–52.
- Bumbacea R, Corcea S, Ali S, Dinica L, Fanfaret I, et al. Mite allergy and atopic dermatitis: Is there a clear link? (Review). Experimental and Therapeutic Medicine, (2020); 20: 3554–60.
- Adji A, Niode NJ, Memah V v., Posangi J, Wahongan GJP, et al. Designing an epitope vaccine against Dermatophagoides pteronyssinus: An in silico study. Acta Tropica, (2021); 222.
- Anggraeni S, Damayanti D, Umborowati MA, Riswanto CD, Rhatomy S, et al. Efficacy and safety of specific immunotherapy with aeroallergens in the management of atopic dermatitis. International Journal of Health Sciences, (2022); 6(S9): 2444–61.
- Jutel M, Solarewicz-Madejek K, Węgrzyn A. Allergen-specific immunotherapy in atopic dermatitis. Postępy Dermatologii Alergologii XXVII, (2011); 5: 389–95.
- Shin JU, Kim SH, Noh JY, Kim JH, Kim HR, et al. Allergen-specific immunotherapy induces regulatory T cells in an atopic dermatitis mouse model. Allergy, (2018); 73(9): 1801–11.
- Bencze J, Szarka M, Kóti B, Seo W, Hortobágyi TG, et al. Comparison of semi-quantitative scoring and artificial intelligence aided digital image analysis of chromogenic immunohistochemistry. Biomolecules, (2022); 12(1).
- Fedchenko N, Reifenrath J. Different approaches for interpretation and reporting of immunohistochemistry analysis results in the bone tissue – a review. Diagnostic Pathology, (2014); 9: 221.
- Shershakova N, Bashkatova E, Babakhin A, Andreev S, Nikonova A, et al. Allergen-Specific Immunotherapy with Monomeric Allergoid in a Mouse Model of Atopic Dermatitis. PLoS One, (2015); 10(8): e0135070.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0