

Full Length Research Article
Differential molecular detection of seasonal influenza A viruses in suspected patients of COVID-19
Roaa Abdulla Sabeeh1, Firas Taha Mansour Al-Mubarak1*, Alaa Khattar Mousa2
Adv. life sci., vol. 12, no. 2, pp. 346-350, May 2025
*– Corresponding Author: Firas Taha Mansour Al-Mubarak (Email: firasiraqi76@gmail.com)
Authors' Affiliations
2. Department of Internal Medicine, College of Medicine, University of Basrah, Basrah – Iraq
[Date Received: 20/10/2024; Date Revised: 05/01/2025; Available Online:22/03/2025; Date Updated: 31/08/2025]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Seasonal influenza greatly affects the health of the community, resulting in many hospitalizations and, in some cases, even deaths. In our geographic area, obtaining accurate statistics on seasonal influenza infection rates has been challenging, particularly during the ongoing COVID-19 pandemic. The aim of this study is to investigate seasonal influenza virus infections in the community of Basrah, southern Iraq.
Methods: A total of 820 nasopharyngeal swabs were collected from people with clear respiratory symptoms of different age groups, and of both sexes during the period from the 1st of October 2021 to the 1st of May 2022. This cross-sectional study included four important districts in the province of Basrah, which are the city center, Abulkhasib, Shatt Al Arab, and Al-Zubair. All samples were subjected to viral RNA extraction and detection by one-step RT-PCR using a pair of universal primers.
Results: According to the results obtained, the total infection rate in the study areas reached 19.5%. There were no differences in infection rates between the sexes. The age groups of the study showed that the youngest group (1-9 years) recorded the highest infection rate (30.6%), while the group with the lowest infection rate was within the 40-49 age group, which was 16%. In addition, October and April showed the lowest number of infections compared to other months, which extended from November to the end of April.
Conclusion: These results give a general picture of seasonal influenza infection rates in our geographical location, as there is an urgent need to update this information, especially during the ongoing coronavirus pandemic.
Keywords: Seasonal influenza; RT-PCR; Iraq
Introduction![]()
Influenza A viruses, which belong to the Orthomyxoviridae family, are enveloped with surface glycoprotein spikes, and their genome involves 8 single-stranded RNA segments [1]. These viruses have the potential to infect a wide variety of animal species, including humans, birds, and several other mammals [2]. They have been determined to cause seasonal (annual) influenza outbreaks and serious occasional pandemics. They cause a range of diseases in humans during the winter months in all regions of the world, ranging from mild to severe respiratory symptoms, and sometimes with serious complications [3]. Common symptoms include fever, sore throat, cough, body aches, fatigue, and respiratory congestion. In some cases, notably in immunocompromised patients, secondary bacterial infections, and severe influenza infections can lead to pneumonia, organ failure, and even death [4].
Based on two surface proteins, hemagglutinin (H) and neuraminidase (N), influenza A viruses are classified into various subtypes. Currently, there are 18 H subtypes (H1 to H18) and 11 N subtypes (N1 to N11). These subtypes contribute to identifying different strains of influenza A viruses. The incorporation of specific H and N subtypes determines the strain of the influenza A virus [5]. For instance, the H1N1, and H3N2 subtypes are common strains that cause seasonal influenza outbreaks in humans [6,7], and the H5N1 is an important subtype for birds that occasionally transmit to humans [8]. Although there is an effective vaccine against seasonal influenza, yearly update of seasonal influenza vaccines is necessary because of the continuous evolution of influenza viruses [9]. While there is more than one virus subtype responsible for seasonal influenza, it is beneficial that the virus can be detected in the community without the need for virus subtyping. This can be done using a set of universal PCR primers capable of capturing any influenza A virus infection [10].
Respiratory diseases in humans have several causes, some of which are bacterial and others viral. The most important bacterial causes are Streptococcus, Haemophilus, Mycoplasma, Corynebacterium, and Bordetella [11]. The most important viral causes include influenza viruses A and B, coronaviruses, respiratory syncytial virus, Rhinovirus, adenovirus, and human metapneumovirus [12,13]. These pathogens commonly manifest during the autumn and winter seasons, where they are in close proximity to each other, it becomes crucial to promptly investigate their cause through accurate methods. This ensures that patients receive the appropriate treatment based on a precise diagnosis. On the other hand, the occurrence of repeated waves of the global COVID-19 pandemic has posed significant challenges to the diagnosis process. The presence of striking clinical similarities with other respiratory illnesses has caused substantial confusion [14,15].
In our specific region, relatively few studies have been conducted regarding human-to-human transmission of seasonal influenza viruses, particularly during the ongoing coronavirus pandemic. Due to the large number of respiratory infections in our geographical regions, especially in the months when the weather is relatively moderate to cold, the inclusion criteria were to include all patients suffering from these respiratory infections. The study aims to investigate the presence of influenza viruses in general, regardless of their subtypes. This will give us a comprehensive idea of the percentage of influenza virus illnesses compared to other respiratory infections.
Methods![]()
Sample collection
During the period from the 1st of October 2021 to the 1st of May 2022, a total of 820 nasopharyngeal swabs were collected from individuals exhibiting symptoms of influenza such as high body temperature (above 38°C), cough, shortness of breath, sore throat, and pneumonia. The samples were collected from 4 districts in Basrah as follows: 388 samples from the city center, 170 samples from Abulkhasib, 135 samples from Shatt Al Arab, and 127 samples from Al-Zubair. The samples were divided into 7 age groups starting from 1-9 to 60-69 years old with both males and females. The collected samples were directly put in tubes containing virus transport media (VTM) and then shipped to the laboratory in cold conditions to prepare for RNA extraction.
Viral RNA extraction and quantification
The samples were subjected to viral RNA extraction using QIAamp Viral RNA Mini Kit supplied by Qiagen following the instructions provided by the manufacturer. The yielded RNA was quantified using a NanoDrop spectrophotometer to identify its quality and quantity. The RNA was subsequently stored in a freezer at a temperature of -20˚C until it was ready for further use.
Conventional RT-PCR and gel electrophoresis
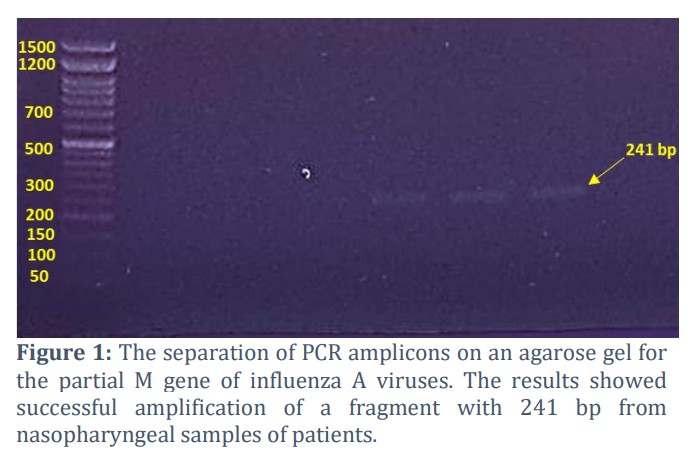
The Bioneer's One-Step RT-PCR kit was used for the amplification of all gene fragments included in the study. To detect suspected cases of seasonal influenza, a forward GGGACTCATCCTAGTTCCAGTA and a reverse CTCAGGTACTCCTTCCGTAGAA universal primer set were designed using the tools available on NCBI to amplify an amplicon with a size of 241 base pair within the viral M gene. The initial RNA concentration that was used as starting material for cDNA synthesis was a concentration of 150 ng/μl. The conditions of RT-PCR utilized were as follows: the synthesis step of the complementary DNA (cDNA) was conducted at 45°C for 30 min. Following that, an initial denaturation step was done at 94°C for 5 min. Then, a total of 40 DNA amplification cycles were achieved, represented by denaturation at 94°C for 15 sec, annealing at 59°C for 30 sec, and extension at 72°C for 1 min. Following these cycles, the final elongation step was performed at 72°C for 1 min. At the end of the mentioned steps, the reaction was held at 4°C for 10 min. To detect PCR products, a gel made of 1.5% agarose dissolved in TAE buffer, and stained with Nancy-520, was used. The PCR product (10 μl for each sample) was loaded into each well on the gel. The amplicon size was estimated by comparing it to a standard DNA ladder.
Ethical consideration
All work and analyzes were carried out following the guidelines approved by the College of Medicine, University of Basra/Iraq.
Results![]()
Molecular detection of seasonal influenza A virus
Out of the 820 samples tested, 160 of them (19.5%) were positive for the influenza A virus and 660 samples (80.5%) were negative. The results were considered positive after observing clear bands on an agarose gel following the use of the universal primer of the M gene. Figure 1 illustrates the M gene amplification utilizing RT-PCR.
Demographical distribution
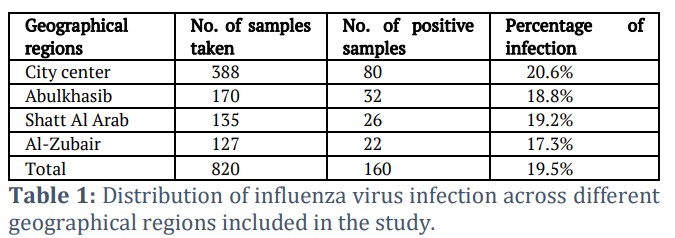
With regard to the geographical distribution of tested samples, the study covered multiple regions in Basrah, and the percentage of infection ranged from 17.3% to 20.6% as follows: City center (20.6%), Abulkhasib (18.8%), Shatt Al Arab (19.2%), and Al-Zubair (17.3%) (Table 1).
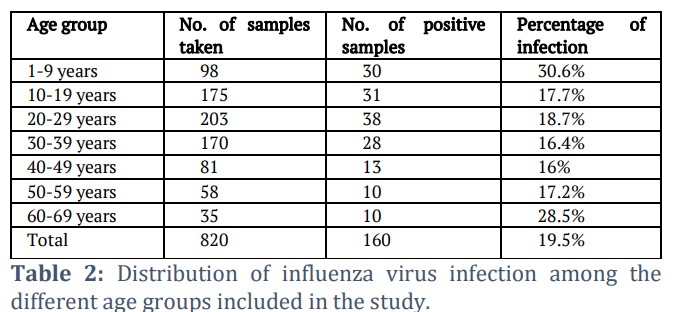
In terms of the distribution of the results according to the age groups included in the study, the lowest rate of infection was 16% in the age group 40-49 years, and the highest rate of infection was 30.6% in the age group 1-9 years. The details of the rate of infection among the other age groups are shown in Table 2.
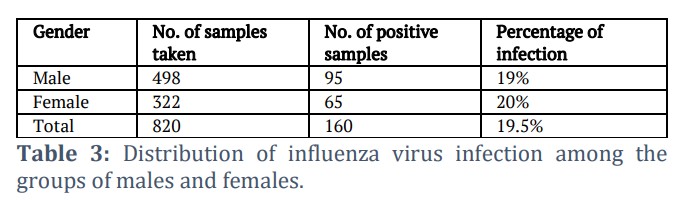
Regarding the sex of the patient, the percentage of infection among the male and female groups was similar, which were 19% and 20%, respectively (Table 3). This result suggests that the incidence of the disease is not a gender-related preference.
Seasonal variation in disease distribution
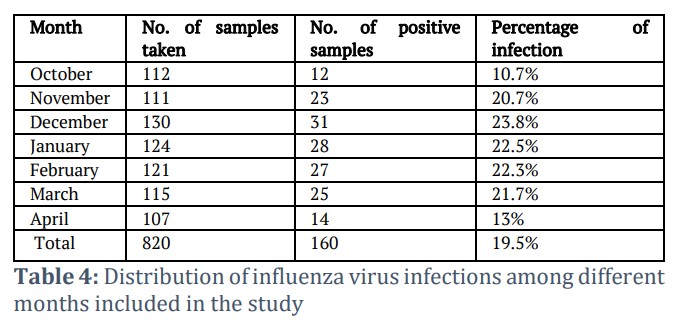
With regard to disease prevalence according to the study period, October and April exhibited the lowest rates among the months included in the study. The ratio of infections in October was 10.7%, and in April was 13%. In comparison, the infection rate in the other months ranged from 20.7% to 23.8% (Table 4).
Figures & Tables
The primary measure in controlling infectious diseases is to establish a foundation for reliable and precise diagnosis. This step is crucial for identifying the accurate pathogen and excluding the other potential causes. This is considered necessary, especially during the period of the COVID-19 pandemic, as the disease is spreading in all countries of the world [16,17]. In this study, we conducted a general survey to detect seasonal influenza viruses during their peak period from the beginning of October to the end of April. We concluded through this study that the total incidence of seasonal influenza was 19.5% of the total respiratory infections. The remaining percentage may be shared between the pandemic virus and other respiratory infections, which are endemic in our region and the rest of the world.
In this study, a pair of universal primers were used to screen influenza viruses, in general, using the RT-PCR technique. Molecular methods, particularly RT-PCR, have been widely used to detect influenza viruses due to their high sensitivity and specificity [18,19]. Therefore, this assay was chosen to obtain collective results from seasonal influenza infections. Although there are different serological tests to detect the influenza virus, cross-reactions with other viruses can happen and eventually give false positive results, which might affect the overall infection rate [20,21].
In this study, there were two factors that did not have an effect on the incidence of seasonal influenza. These were the geographical distribution of patients and their sexes. The increasing similarity between regions in terms of urban growth, access to health care, and population diversity in recent years may be the reason for the apparent similarity in the geographic distribution of influenza cases. Before the current decade, when health care was limited in rural areas, this diversity did not exist. Furthermore, although several studies found there is little association between the gender of the patient and infection with seasonal influenza, our findings suggest that there was no significant association between sexes. There may be a disparity in the rate of hospital admissions, with a higher occurrence among women, particularly pregnant women, compared to men [22]. However, another study revealed that the infection rate is slightly higher in males compared to females [23]. The mechanisms underlying the sex differences may involve many factors such as immunological, hormonal, behavioral, and genetic factors.
Regarding age groups, based on the findings obtained in our study, it was clear that the highest rates of infection were in two specific age groups. The first group includes children aged 1 to 9 years, and the second group included individuals aged 60 to 69 years. This is in line with a study that found people ages 65 and older have a greater chance of developing serious flu-related symptoms and consequences. The presence of chronic diseases and decreased immune function are reasons for increased susceptibility to infection [24]. Another study also indicated that the burden of influenza is not distributed equally between different age groups, as children under the age of five suffer from more serious consequences than older children and adults [25], and this in turn is consistent with the results we obtained in our study. In addition, regarding infection rates by infection season, our data showed that compared to other months, infection rates were lower in October and April. The reason for this seasonal variation requires further investigation, as the observation of lower infection rates during months with cooler temperatures is contrary to the established knowledge that influenza virus stability and transmission are typically enhanced under such conditions. These results are consistent with most of our neighboring countries, as well as with the other countries in the world [26,27]. In the meantime, it is important to realize that these results may undergo slight modifications due to the ongoing effects of climate change.
Taken together, these results provide important new information about seasonal influenza infection rates. It is worth noting that there was no difference in the detected infection rate according to the patient's sex or geographical location. Furthermore, older and younger patient groups have the highest infection rates.
Author Contributions
Roaa Abdulla Sabeeh: Was responsible for sample collection, table design, and participated in laboratory work, editing and writing.
Firas Taha Mansour Al-Mubarak: Participated in research and all stages of laboratory work, editing and writing.
Alaa Khattar Mousa: Participated in article editing and writing the final version of the article. ![]()
References
- Bouvier NM, Palese P. The biology of influenza viruses. Vaccine, (2008); 4(Suppl 4): D49-53.
- Zhang M, Liu M, Bai S, Zhao C, Li Z, et al. Influenza A Virus-Host Specificity: An Ongoing Cross-Talk Between Viral and Host Factors. Frontiers in Microbiology, (2021);12: 777885
- Feldblyum TV, Segal DM. Seasonal and Pandemic Influenza Surveillance and Disease Severity. Global Virology I – Identifying and Investigating Viral Diseases, (2015); 12: 761–89.
- Morris DE, Cleary DW, Clarke SC. Secondary Bacterial Infections Associated with Influenza Pandemics. Frontiers in Microbiology, (2017); 8: 1041.
- Kosik I, Yewdell JW. Influenza Hemagglutinin and Neuraminidase: Yin⁻Yang Proteins Coevolving to Thwart Immunity. Viruses, (2019); 11(4): 346.
- Allen JD, Ross TM. H3N2 influenza viruses in humans: Viral mechanisms, evolution, and evaluation. Human Vaccines & Immunotherapeutic, (2018); 14(8): 1840-1847.
- Dotis J, Roilides E. H1N1 influenza A infection. Hippokratia, (2009); 13(3): 135-138.
- Peiris JS, de Jong MD, Guan Y. Avian influenza virus (H5N1): a threat to human health. Clinical Microbiology Reviews, (2007); 20(2): 243-267.
- Nuwarda RF, Alharbi AA, Kayser V. An Overview of Influenza Viruses and Vaccines. Vaccines, (2021); 9(9): 1032.
- Hoffmann E, Stech J, Guan Y, Webster RG, Perez DR. Universal primer set for the full-length amplification of all influenza A viruses. Archives of Virology, (2001); 146(12):2 275-289.
- Metzger DW, Sun K. Immune dysfunction and bacterial coinfections following influenza. The Journal of Immunology, (2013); 191(5): 2047-2052.
- Kesson AM. Respiratory virus infections. Pediatric Respiratory Review, (2007); 8(3): 240-248.
- Khadadah M, Essa S, Higazi Z, Behbehani N, Al-Nakib W. Respiratory syncytial virus and human rhinoviruses are the major causes of severe lower respiratory tract infections in Kuwait. Journal of Medical Virology, (2010); 82(8): 1462-1467.
- Ljubin-Sternak S, Meštrović T, Lukšić I, Mijač M, Vraneš J. Seasonal Coronaviruses and Other Neglected Respiratory Viruses: A Global Perspective and a Local Snapshot. Frontiers in Public Health, (2021); 9: 691163.
- Parry MF, Shah AK, Sestovic M, Salter S. Precipitous Fall in Common Respiratory Viral Infections During COVID-19. Open Forum Infectious Diseases, (2020); 7(11): 511.
- Van Seventer JM, Hochberg NS. Principles of Infectious Diseases: Transmission, Diagnosis, Prevention, and Control. International Encyclopedia of Public Health, (2016): 22–39.
- Wang C, Liu M, Wang Z, Li S, Deng Y, et.al. Point-of-care diagnostics for infectious diseases: From methods to devices. Nano Today, (2021); 37: 101092.
- Otto CC, Kaplan SE, Stiles J, Mikhlina A, Lee C, et al. Rapid Molecular Detection and Differentiation of Influenza Viruses A and B. Journal of Visualized Experiment, (2017); (119): 54312.
- Yarbrough ML, Burnham CD, Anderson NW, Banerjee R, Ginocchio CC, et al. Influence of Molecular Testing on Influenza Diagnosis. Clinical Chemistry, (2018); 64(11): 1560-1566.
- Khan S, Nakajima R, Jain A, de Assis RR, Jasinskas A, et al. Analysis of Serologic Cross-Reactivity Between Common Human Coronaviruses and SARS-CoV-2 Using Coronavirus Antigen Microarray. bioRxiv [Preprint], (2020): 006544.
- Chen YQ, Wohlbold TJ, Zheng NY, Huang M, Huang Y, Neu KE, et al. Influenza Infection in Humans Induces Broadly Cross-Reactive and Protective Neuraminidase-Reactive Antibodies. Cell, (2018); 173(2): 417-429.
- Kline K, Hadler JL, Yousey-Hindes K, Niccolai L, Kirley PD, et al. Impact of pregnancy on observed sex disparities among adults hospitalized with laboratory-confirmed influenza, FluSurv-NET, 2010-2012. Influenza and Other Respiratory Viruses, (2017); 11(5): 404-411.
- Aufi IM, Khudhair AM, Ghaeb Al-Saadi L, Almoneem Ahmed MA, Mahdi Shukur FM. Epidemiology and Molecular Characterization of Seasonal Influenza Viruses in Iraq. Archives of Razi Institute, (2021); 76(4): 871-877.
- Langer J, Welch VL, Moran MM, Cane A, Lopez SMC, et al. High Clinical Burden of Influenza Disease in Adults Aged ≥ 65 Years: Can We Do Better? A Systematic Literature Review. Advances in Therapy, (2023); 40(4): 1601-1627.
- Ruf BR, Knuf M. The burden of seasonal and pandemic influenza in infants and children. European Journal of Pediatrics, (2014); 173(3): 265-276.
- Caini S, El-Guerche Séblain C, Ciblak MA, Paget J. Epidemiology of seasonal influenza in the Middle East and North Africa regions, 2010-2016: Circulating influenza A and B viruses and spatial timing of epidemics. Influenza and Other Respiratory Viruses, (2018); 12(3): 344-352.
- Radhi AH, Ibrahim ZH, Alhilifi R. The epidemiological pattern of seasonal influenza in four sentinel sites in Iraq. Influenza Other Respiratory Viruses, (2023); 17(4): e13134.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0