

Full Length Research Article
Characterization of Mutations Linked with Second Line Anti-TB Drug Resistance in Pakistan
Riffat Jabeen1, Memona Yasmin1, Hafiza Rabia Dar2, Rubina Tabassum Siddiqui3*, Inaam Ullah1
Adv. life sci., vol. 8, no. 2, pp. 137-142, February 2021
*- Corresponding Author: Rubina Tabassum Siddiqui (Email: tabassum.rubina@gmail.com)
Authors' Affiliations
2. Medical Biochemistry Research Laboratory, Department of Biochemistry, University of Agriculture, Faisalabad – Pakistan
3. Punjab Institute of Nuclear Medicine (PINUM), Faisalabad – Pakistan
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: The incidence of multiple drug resistance tuberculosis is on the rise worldwide and Pakistan is one of 30 high TB burden countries. Resistance to second line drugs especially fluoroquinolones is being reported by many laboratories. This is increasing the gravity of the situation resulting in extensively drug resistant cases, which is difficult to treat, and has more side effects.
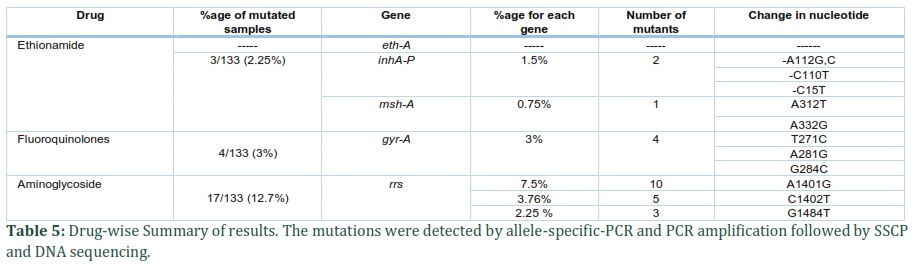
Methods: One hundred and thirty-three (133) clinical isolates of M. tuberculosis, collected by convenience sampling, were characterized for mutations in eth-A, gyrA, msh-A, rrs genes, and the promoter region of inh-A gene that confer resistance to second line anti-TB drugs. The mutations were detected by allele-specific-PCR and PCR amplification followed by SSCP and DNA sequencing.
Results: Mutations in gyrA gene at codon 91, 94 and 95 were found in 4 (3.0%) M. tuberculosis isolates. Mutations in rrs gene were found in 17 (12.8%) isolates, ten (7.5%) isolates had mutation at A1401G position, 5 (3.76%) isolates at C1402T position and 3 (2.25%) isolates had G1484T mutation. For resistance to ethionamide, none of the isolates showed mutation in eth-A gene. In promoter region of inh-A gene, mutations were detected at -C15T, -A112G, -C110T in two samples. Two mutations, A312T and A332G, were found in msh-A gene in one sample. Collectively, 24 (18%) isolates were found to harbor mutations associated with second line anti TB drug resistance.
Conclusion: Our work revealed high frequency of mutations (18%) associated with resistance against second line anti-TB drugs. This situation can lead to increase in XDR-TB cases. We, therefore, recommend improved diagnostic and drug sensitivity testing, better prescription, and development of superior drugs to control tuberculosis.
Keywords: Antibiotic resistance; Mycobacterium tuberculosis; Second line anti-TB drugs
Introduction![]()
Tuberculosis (TB) is an air born disease caused by Mycobacterium tuberculosis (M. tuberculosis). Mostly, it affects lungs (pulmonary TB) but other sites of the body could also get affected causing extrapulmonary TB. It is one of the top 10 causes of death worldwide with an estimated 10.0 million incident cases and 1.2 million deaths. According to World Health Organization report of 2020, drug resistant tuberculosis is continuously a public health threat and is obstacle to TB care and prevention. The incident of rifampicin-resistant TB (RR-TB) in 2019 is reported to be half a million people, of which 78% had multidrug resistant TB (MDR-TB) [1]. MDR-TB is defined as resistance to rifampicin (RIF) and isoniazid (INH) with or without resistance to the other first-line anti-TB drugs. On the other hand, incident of extensively drug resistant TB (XDR-TB) accounts 7.4% of MDR-TB globally [2]. XDR-TB is defined as MDR-TB with resistance to any fluoroquinolones and at least one of the second-line injectable – amikacin, capreomycin or kanamycin anti-TB drugs. The actual incidence may be higher than the reported cases because many low and lower middle-income countries do not have adequate capability to test for resistance to second-line drugs and thus to detect XDR-TB.
Pakistan ranks 5th among 8 “high TB burden” countries having two third of all estimated incident cases worldwide. According to National TB Control Program, 580,000 new cases of all forms of TB are reported annually with 50,000 deaths. Moreover, there are estimated 28,000 reported cases of MDR-TB where only 11% of them were diagnosed and treated [3]. These patients will receive second line anti-TB drug therapy including fluoroquinolones (FQ), a vital component of drug regimen for MDR cases. Treatment of MDR-TB is more challenging as it relies on prolonged use of second line anti-TB drugs while XDR-TB treatment is further hampered by use of more toxic, less effective and expensive anti-TB drugs including use of longer duration of injectable drugs. Recently, van der Heijden et.al., [4] has reported an increase in FQ resistance in anti TB treatment-naive TB patients that lead to increased mortality.
Fluoroquinolones disrupt the function of gyrA and gyrB genes that consequently ceases bacterial growth. Mutations in these genes make these drugs ineffective against bacteria. The most commonly found missense mutations are at position 90, 91 and 94 in gyrA gene [5]. The second-line anti-TB drugs apart from FQ and streptomycin are aminoglycosides (capreomycin (CM), amikacin (AK), kanamycin (KM)) and ethionamide (ETA). Capreomycin is peptide in nature and inhibits protein synthesis by binding with 50S or 30S ribosomal RNA. Mutations in rrs gene and tly-A gene are associated with resistance against aminoglycosides. Ethionamide is a pro-drug which becomes active with the help of an enzyme, monooxygenase [6,7]. This enzyme is coded by the gene eth-A which is regulated by eth-R [8]. After activation, these drugs target the activity of ndh-A, inh-A and msh-A genes which are involved in the synthesis of bacterial cell wall.
Drug susceptibility in M. tuberculosis strains is conventionally based on culture in liquid or solid media. Though it adequately detects RIF or INH resistance but is less reliable and complicated for second line anti-TB drugs [9]. Moreover, many developing countries do not have the resources to establish the facility for drug susceptibility testing for second line anti-TB drugs. These growth-based methods require weeks to months and the patients resistant to these drugs remain contagious and may die before they are treated with right medicines. Further, these infected and uncured patients remain a potent source of transmission of drug resistant form of disease in the community. The advent of molecular biology techniques that do not require culturing these slow-growing pathogens are helpful in the management of M/XDR-TB.
We, hereby, report mutations associated with second line anti-TB drug resistance in M. tuberculosis isolates from Pakistan.
Methods![]()
Sample Collection
In total, 133 M. tuberculosis isolates were collected by convenience sampling from TB patients belonging to different cities of Pakistan. Twenty-five culture isolates were collected from Armed Forces Institute of Pathology, seven from Mayo Hospital Lahore and six from TB hospital Faisalabad. DNA from ninety-five M. tuberculosis isolates was provided by Holy Family Hospital, Rawalpindi. Clinical specimens were cultured on Lowenstein Jenson (LJ) media. DNA extraction was performed using CTAB method [10].
PCR Amplification
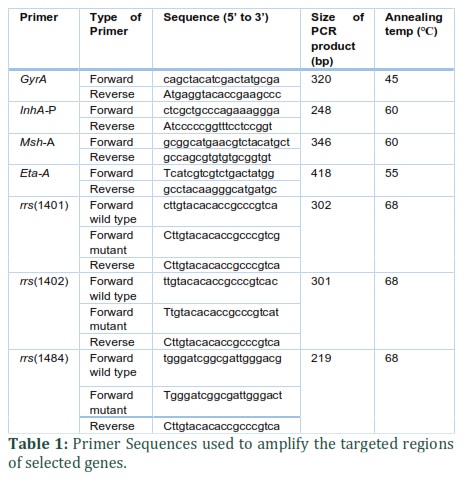
The primers were designed for the promoter region of inh-A gene and for the hot spot regions of msh-A and eth-A gene. The primers for the gyrA gene were retrieved from a previous study [11]. The primers for ASO-PCR of three most common mutations (A1401G, C1402T, G1484T) in rrs gene were also designed. Primers for all these targeted regions were synthesized based on NCBI reference sequence NC_000962.3 of M. tuberculosis H37Rv. The PCR primer sequences, annealing temperatures and the size of the amplification products are listed in table 1. PCR products were analyzed by agarose gel electrophoresis.
Single stranded conformational polymorphism (SSCP) analysis
PCR products of hotspot regions of gyrA, mshA, inhA, and eth-A genes were resolved on 7% polyacrylamide gel for single strand confirmation polymorphism (SSCP) analysis. The amplified hotspot regions of the isolates that showed mobility shift in SSCP analysis were sequenced commercially.
Allele specific oligonucleotide (ASO) PCR analysis
For the detection of most common mutations (A1401G, C1402T, G1484T) in rrs gene, ASO-PCR analysis was done. ASO-PCR amplification products were resolved by agarose gel electrophoresis. The relative absence or presence of the amplification with corresponding primers suggested presence of wild type or mutant allele. The PCR primer sequences, annealing temperature and the size of the amplification products are listed in table 1.
Ethical use statement
Sample collection, experiments and data use were performed under institutional ethical guidelines. No personal details of the patients were disclosed.
Results![]()
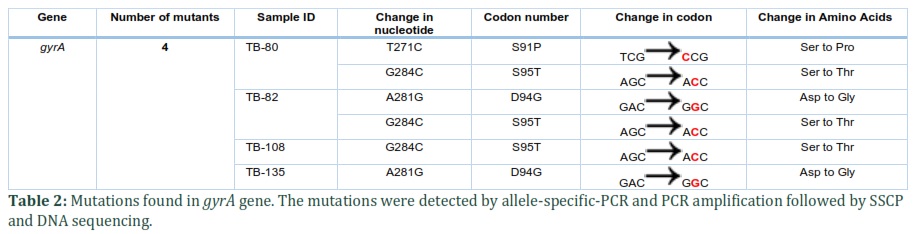
Out of 133 isolates, 4 isolates showed mobility shift in SSCP analysis. Sequencing of these isolates revealed mutations, either singly or in combination, at codon 91, 94 and 95 of gyrA gene. Hence, the frequency of mutations that confer fluoroquinolone resistance was found to be 3.0%. One isolate showed mutations in codons 94 and 95; at codon 94 nucleotide A is changed into G, which results in the replacement of aspartate with glycine, and at codon 95 where G is replaced by C, amino acid serine is replaced by threonine. One isolate harbored mutations at two different codons 91 and 95; at codon 91 nucleotide T is replaced by C and consequently serine is changed into proline and at codon 95 G is replaced by C, amino acid serine is changed into threonine. Two other isolates revealed mutation singly in codon 95 or in codon 94 (table 2).
Ethionamide
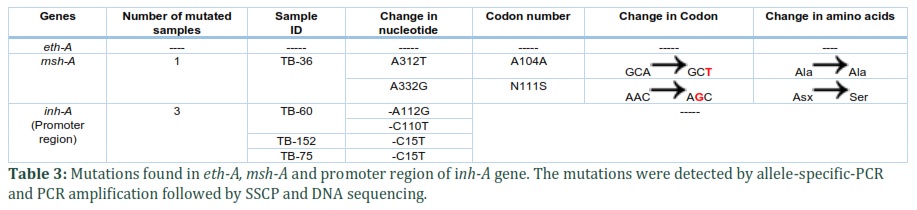
For resistance to ETA, the genes eth-A, msh-A, and complete promoter region of ih-A were characterized. Sequencing results of PCR products revealed no mutation in targeted fragment (418 bp) of eth-A gene. In promoter region of inhA gene -C15T, the most commonly reported mutation, was found in two isolates while two novel mutations (-A112G, -C110T) were observed in one isolate. Thus, collectively, 2.26% isolates showed mutation in promoter region of inh-A. DNA sequencing of 346 bp region of msh-A gene revealed two mutations (A312T, A332G) in one (0.75%) isolate, and among these mutations A312T is a novel mutation (table 3). Collectively, we found 4/133 (3.0%) mutant isolates against ethionamide in inh-A and msh-A genes (Table 3).
Aminoglycosides
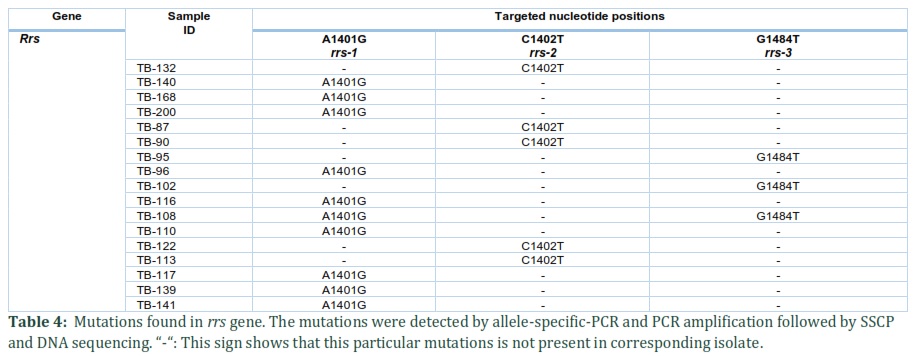
For amikacin, kanamycin and capreomycin drug resistance, three nucleotide positions were targeted by designing ASO primers. PCR and agarose gel electrophoresis results confirmed mutations in rrs gene. These mutations conferring resistance to aminoglycosides, were found in 12.8% (17/133) M. tuberculosis isolates. Ten isolates (7.5%) had mutation at A1401G, 5 isolates (3.76%) at C1402T position, and 3 isolates (2.25%) had mutation at G1484T position. Among these, one sample showed mutations in two codons (A1401G and G1484T). We report the overall mutation frequency of 9.77% against amikacin and kanamycin and 13.53% against capreomycin in M. tuberculosis isolates (Table 4).
Summary of results
In total, we found 24 (18%) mutant isolates in msh-A, promoter region of inh-A, gyrA, and rrs gene, known to confer resistance against second line anti-TB drugs. This is an alarmingly high frequency of mutations in M. tuberculosis strains circulating presently among TB patients in Pakistan. This high frequency of mutations is leading to a disquieting increase in XDR-TB in Pakistan. In this study, four isolates were mutated in gyrA, two were mutated in inh-A, one in msh-A and 17 samples were found mutated in rrs gene (Table 5).
Figures & Tables
Discussion![]()
Fluoroquinolones are an integral component of second-line therapy for multidrug-resistant strains and its resistance is increasing in MDR-TB strains [11]. In the present study, the frequency of mutations in gyrA gene was 3.0%. All these mutations are missense and have already been reported [12]. Our results are in agreement to a previous report from Pakistan where 3.1% of isolates, susceptible to all first-line agents, were reported to be fluoroquinolone resistant [13]. The reason for this may be the extensive use of fluoroquinolones. The fluoroquinolones, being broad spectrum antibiotics, are used for treating several infectious diseases. Their easy administration and excellent gastrointestinal absorption, tissue penetration and lack of unwanted side effects [14] make them the drug of choice for many health practitioners. In Pakistan, fluoroquinolones are available to the general population as over-the-counter medicine and hence its misuse can lead to drug resistance. Moreover, in the absence of strict guidelines for treatment, the physicians overprescribe these drugs. Acquisition of de novo mutations in its target may have a selective pressure to develop FQ resistant bacteria and if this selective pressure extends beyond the targeted etiological agent, it may result in FQ resistant M. tuberculosis strains. Increase in FQ resistant M. tuberculosis strains has also been reported from India (from 3% to 35%) [15] and Taiwan (from 7.7% to 20%) [16].
Mutations in inh-A promoter region were found at three distinct positions where two mutations, -A112G, -C110T are novel. Similarly, DNA sequencing of msh-A revealed novel mutation at A312T. The role of these mutations in drug resistance needs to be elucidated by further studies. Similar mutations within the ethA and inhA structural genes that confer ethionamide resistance have been reported in 49.6% ethionamide resistant M. tuberculosis isolates from India [17], 76% from USA [8] and 56% from Kenya [18]. We found 17 isolates with mutation in rrs gene at targeted positions (A1401G, C1402T and G1484T). Mutations in rrs gene have been reported, in literature, at different nucleotide positions such as, T16G, T16A, C491T, C512T, A513C, C904A, G1302A [19] and 514, 517, 1401, 1402, 1443, 1473, 1484, 152 [20]. A strong correlation has been reported between a mutation at position A1401G and the resistance to amikacin and kanamycin [21-23]. It is reported that the C1402T mutation in the rrs gene is associated with capreomycin resistance and the mutation at G1484T is associated with amikacin, kanamycin and capreomycin resistance [24]. Based on our results, we can deduce that 9.77% isolates harbored mutations associated with amikacin and kanamycin resistance, and 13.53 % with capreomycin resistance. This high frequency of mutations emphasizes the need to design the personalized drug regimen for TB patients carefully, depending upon the drug sensitivity data. Molecular genotypic methods of drug sensitivity testing may be a better option and can complement the phenotypic DST results.
At least 23 countries in Africa and Asia introduced shorter MDR-TB regimens, which have achieved high treatment success rates (87‒90%) under operational research conditions. Based on these studies, WHO now recommends a standardized shorter MDR-TB regimen for selected MDR/RR-TB patients who do not have resistance to fluoroquinolones or second-line injectable agents. In this scenario, it is important to detect the FQ sensitivity of individual patients before starting this more effective and shorter MDR-TB regimen. Genotypic detection of drug sensitivity may help prescribe the appropriate drug regimen for individual patients before the availability of phenotypic DST results. This may contribute in controlling transmission of drug-resistant TB.
Our data shows high frequency of mutations in M. tuberculosis isolates circulating presently among TB patients in Pakistan. We are of the view that the MDR-TB strains in patients starting second-line drug treatment are first tested for sensitivity to these drugs for timely and effective treatment of these patients and to ensure that resistance is not further amplified. This will decrease the incidence and spread of XDR-TB. If the sources allow, we recommend that at least drug sensitivity testing of fluoroquinolones and aminoglycosides should be included when the drug sensitivity against first line anti-TB drugs is being done. Furthermore, genotypic drug sensitivity testing could be a better choice before starting therapy.
Author Contributions
Riffat Jabeen: Sample preparation, DNA extraction, PCR, experiment and write up
Memona Yasmin: Sample collection, SSCP analysis, data analysis, write up, editing
Hafiza Rabia Dar: Write up and review
Inaam Ullah: Data analyses, manuscript editing and submission
Rubina Tabassum Siddiqui: Idea, supervision, data analyses, editing
Acknowledgment
This work is part of Master of Philosophy (M.Phil.) thesis of Ms. Riffat Jabeen. We are thankful to Dr. Shahid Mansoor SI (Director NIBGE) for his help in DNA sequencing. We are thankful to Dr. Naeem Akhtar, Holy Family Hospital Rawalpindi; Dr. Shahid A. Abbasi, Armed Forces Institute of Pathology, Rawalpindi; Dr. Rizwan Iqbal, Pakistan Medical Research Council, Lahore and Meezan Laboratory, Faisalabad for providing M. tuberculosis isolates.
Authors declare no conflict of interest in this work. This work was performed under the institutional ethical and biosafety guidelines.
References![]()
- WHO. Global tuberculosis report. World Health Organization. (2020).
- WHO, WHO. Global tuberculosis report. World Health Organization. (2018).
- Brief Report on World TB Day 2020 in Pakistan, https://www.researchgate.net/publication/340565199_Brief_Report_on_World_TB_Day_2020_in_Pakistan
- van der Heijden YF, Maruri F, Blackman A, Holt E, Warkentin J, et al. Fluoroquinolone exposure prior to tuberculosis diagnosis is associated with an increased risk of death. The International Journal of Tuberculosis and Lung Disease, (2012); 16(9): 1162-1167.
- Von Groll A, Martin A, Jureen P, Hoffner S, Vandamme P, et al. Fluoroquinolone resistance in Mycobacterium tuberculosis and mutations in gyrA and gyrB. Antimicrobial agents and chemotherapy, (2009); 53(10): 4498-4500.
- Baulard AR, Betts JC, Engohang-Ndong J, Quan S, McAdam RA, et al. Activation of the pro-drug ethionamide is regulated in mycobacteria. Journal of Biological Chemistry, (2000); 275(36): 28326-28331.
- DeBarber AE, Mdluli K, Bosman M, Bekker L-G, Barry CE. Ethionamide activation and sensitivity in multidrug-resistant Mycobacterium tuberculosis. Proceedings of the National Academy of Sciences, (2000); 97(17): 9677-9682.
- Morlock GP, Metchock B, Sikes D, Crawford JT, Cooksey RC. ethA, inhA, and katG loci of ethionamide-resistant clinical Mycobacterium tuberculosis isolates. Antimicrobial agents and chemotherapy, (2003); 47(12): 3799-3805.
- Georghiou SB, Magana M, Garfein RS, Catanzaro DG, Catanzaro A, et al. Evaluation of genetic mutations associated with Mycobacterium tuberculosis resistance to amikacin, kanamycin and capreomycin: a systematic review. PloS one, (2012); 7(3): e33275.
- Somerville W, Thibert L, Schwartzman K, Behr MA. Extraction of Mycobacterium tuberculosis DNA: a question of containment. Journal of clinical microbiology, (2005); 43(6): 2996-2997.
- Bozeman L, Burman W, Metchock B, Welch L, Weiner M, et al. Fluoroquinolone susceptibility among Mycobacterium tuberculosis isolates from the United States and Canada. Clinical infectious diseases, (2005); 40(3): 386-391.
- Giannoni F, Iona E, Sementilli F, Brunori L, Pardini M, et al. Evaluation of a new line probe assay for rapid identification of gyrA mutations in Mycobacterium tuberculosis. Antimicrobial agents and chemotherapy, (2005); 49(7): 2928-2933.
- Jabeen K, Shakoor S, Chishti S, Ayaz A, Hasan R. Fluoroquinolone-resistant Mycobacterium tuberculosis, Pakistan, 2005–2009. Emerging infectious diseases, (2011); 17(3): 566.
- Choi S-H, Kim EY, Kim Y-J. Systemic use of fluoroquinolone in children. Korean journal of pediatrics, (2013); 56(5): 196.
- Singhal R, Reynolds PR, Marola JL, Epperson LE, Arora J, et al. Sequence analysis of fluoroquinolone resistance-associated genes gyrA and gyrB in clinical Mycobacterium tuberculosis isolates from patients suspected of having multidrug-resistant tuberculosis in New Delhi, India. Journal of clinical microbiology, (2016); 54(9): 2298-2305.
- Huang T-S, Kunin CM, Shin-Jung Lee S, Chen Y-S, Tu H-Z, et al. Trends in fluoroquinolone resistance of Mycobacterium tuberculosis complex in a Taiwanese medical centre: 1995–2003. Journal of Antimicrobial Chemotherapy, (2005); 56(6): 1058-1062.
- Lakshmi R, Kumar V, Baskaran M, Sundar S, Rahman F, et al. Pattern of ethionamide susceptibility and its association with isoniazid resistance among previously treated tuberculosis patients from India. Brazilian Journal of Infectious Diseases, (2011); 15(6): 619-620.
- Ongaya V, Githui W, Meme H, Kiiyukia C, Juma E. High ethionamide resistance in Mycobacterium tuberculosis strains isolated in Kenya. African Journal of Health Sciences, (2012); 20(1-2): 37-41.
- Leung K, Yip C, Yeung Y, Wong K, Chan W, et al. Usefulness of resistant gene markers for predicting treatment outcome on second‐line anti‐tuberculosis drugs. Journal of applied microbiology, (2010); 109(6): 2087-2094.
- Jugheli L, Bzekalava N, de Rijk P, Fissette K, Portaels F, et al. High level of cross-resistance between kanamycin, amikacin, and capreomycin among Mycobacterium tuberculosis isolates from Georgia and a close relation with mutations in the rrs gene. Antimicrobial agents and chemotherapy, (2009); 53(12): 5064-5068.
- Alangaden GJ, Bone SA. The clinical use of fluoroquinolones for the treatment of mycobacterial diseases. Clinical infectious diseases, (1997); 25(5): 1213-1221.
- Maus CE, Plikaytis BB, Shinnick TM. Molecular analysis of cross-resistance to capreomycin, kanamycin, amikacin, and viomycin in Mycobacterium tuberculosis. Antimicrobial agents and chemotherapy, (2005); 49(8): 3192-3197.
- Taniguchi H, Chang B, Abe C, Nikaido Y, Mizuguchi Y, et al. Molecular analysis of kanamycin and viomycin resistance in Mycobacterium smegmatis by use of the conjugation system. Journal of bacteriology, (1997); 179(15): 4795-4801.
- Suzuki Y, Katsukawa C, Tamaru A, Abe C, Makino M, et al. Detection of kanamycin-resistant Mycobacterium tuberculosis by identifying mutations in the 16S rRNA gene. Journal of clinical microbiology, (1998); 36(5): 1220-1225.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0

