

Review Article
A Review on the impacts of Azadirachta indica on Multi-drug Resistant Extended Spectrum Beta Lactamase-positive of Escherichia coli and Klebsiella pneumonia
Faisal MB. Al-Sarraj
Adv. life sci., vol. 8, no. 3, pp. 228-232, July 2021
*– Corresponding Authors: Faisal MB. Al-Sarraj (Email: falsaraj@kau.edu.sa)
Authors' Affiliations
Abstract![]()
Introduction
Methods
Discussion
Conclusion
References
Abstract
Neem trees have long been considered the holy grail of holistic and nature-based treatments. The medicinal properties that constituents of the trees possess to range from traits that are immunomodulatory to traits combat different disease and infections such as anti-inflammatory and antibacterial effects, to insulating properties that include cardioprotective and hepatoprotective effects. The role of Extended Spectrum Beta-Lactamase positive (ESBL+) bacteria in the occurrence and recurrence of Urinary Tract Infection (UTI) infections, particularly in the Gulf region has been studied extensively. However, suggested treatment methods have had little success due to a variety of factors which include drug resistance, the inability of doctors to calculate the optimal duration for treatment, which has resulted in wrong antibiotic prescriptions, as well as lack of understanding of how UTIs work and thrive in different demographics/ populations which again, results in inappropriate antibiotic treatment of the disease. These discoveries raised the issue of professionals needing better training and education in issues to do with UTIs amongst different demographics of people. In this investigation, the medicinal and pharmacological properties of A. indica from neem leaves were assessed by studying how they affected the activity of ESBL+ bacteria, based on literature from similar studies. The goal and objective of this study were to see if ESBL+ bacteria persisted in the presence of A. Indica from leaf extract, as well as gaining an understanding of the factors that affected the persistence and subsequent treatment of the bacteria using A. indica.
Keywords: Azadirachta indica; Neem; UTI; ESBL; E. coli; K. Pneumoniae
Introduction![]()
Urinary tract infections (UTIs) are pathogenic diseases caused by bacteria traveling up and invading the urinary tract, which extends from the urethra to the bladder. UTIs are of two types: cystitis and pyelonephritis, with cystitis being a lower tract infection confined to the bladder while pyelonephritis is an upper tract infection found in the ureters and kidneys [1].
Colonic bacteria are the most common causes of UTIs, which are mostly members of Enterobacteriaceae family of different species that have other common traits that include being gram-negative, the rod-shaped bacillus that are non-fermenting, facultative and anaerobic in nature [2].
The species' strains that are particularly responsible for persistent UTI infections in different population groups include Escherichia coli (E. coli) and Klebsiella pneumoniae (K. pneumoniae) [1-4].
These species strains are responsible for other common infections such as bacteremia, infections of the central nervous system (CNS), diarrhea as well as severe hospital-acquired infections [2]. However, these no species types also have strains that can produce ESBLs, which can eventually result in antibiotic resistance. Studies conducted in the Gulf and Kingdom of Saudi Arabian (KSA) states explored the occurrence of UTIs in both the pediatric population as well as the male and female adult populations and assessed the effectiveness of using antibiotics to treat these populations.
Literature by Hanna-Wakim [3], which focused on incidence and characteristic features of UTIs in the Lebanese pediatric population, found that in a sample of 675 UTI cases, 77% of those diagnosed were girls. Hanna-Wakim [3] also noted an increasing resistance to cephalosporins and fluoroquinolones by ESBL-producing organisms that were noted to cause the UTIs. In another study on the pediatric population in Jordan by Al-Momani [5], the majority of cases were identified in the age group of 1-5-year-olds and the infections were caused by different species types which were suggested to require different dosage adjustments and/or different methods of treatments. In Qatar, Eltai [6] discovered that dominance by ESBL-producing E. coli and K. pneumoniae gave rise to the need for regulating UTI treatment in children.
According to Alshalat's [7] he targeted on older adults in Qatar revealed that the incidence of UTIs and Catheter-associated UTIs (CA-UTIs), in homecare was especially high, with 132 individuals out of the total sample of 614, being diagnosed with a UTI within the period of the study, which was revealed to be caused by E. coli. Literature by Al Salman [8] showed how inappropriate antibiotic treatment was common in treatments prescribed by ER doctors and how males were prone to receiving these wrong types of treatments because doctors failed to adjust treatment's optimal duration.
All these cases in the literature where wrongful antibiotic treatment was prescribed, made it apparent that there is a need to explore alternative avenues in treating UTIs in both pediatric and adult populations. This has led to the study of the Neem tree and its medicinal properties which produce effects that range from being anti-inflammatory, to immunomodulatory, to antifungal and antibacterial in nature [9,10].
Methods![]()
Literature Search Strategy and Selection Criteria
The study was conducted in Saudi Arabia and Gulf countries. The literature search strategy was done in an orderly and methodical way in Saudi digital library (SDL), Web of Science and PubMed medical databases as they are more frequently used in these Gulf countries. This was to identify publications within the last two decades that are relevant to the review. The search strategy took in all articles encompassing the descriptors, and their structures were advanced in reference to the jargon terms of each database that focused on the abstract and title. The search was conducted on the basis of identifying Gram-negative associated infections and Enterobacteriaceae producing infections. The study was conducted across all age groups. More articles and publications were found in the citations of the former, already identified articles. To be able to locate the associated publications, certain criteria were used. For the criteria, research must have accounted for one pathogenic bacteria genus among the Gram-negative bacteria, must have been conducted with human as subjects of the tests, should have been able to pinpoint bacteria and identify it from the available specimen, and must have been conducted in Saudi Arabia and the Gulf countries and published in English. Consequently, articles and publications that were not conducted in Saudi Arabia and the Gulf countries, and/or those ones that did not focus on any of the criteria used, were exempted. The selection of publications, therefore, was done according to the relevance of titles of the articles of the identified literature and their state on the basis of the inclusion criteria. Contents that matched the inclusion criteria and had been conducted in Saudi Arabia and Gulf countries and had been published in English were assessed and used for this review.
Discussion![]()
Resistant ESBL+ K. pneumoniae infected Urothelial cells and the subsequent UTI
ESBL+ bacteria are bacteria that produce enzymes capable of hydrolyzing penicillin, broad-spectrum cephalosporins and monobactams [11]. These ESBLs are often located on strains that are transferrable from strain to strain and between species [2,11]. E. coli and K. pneumoniae account for 10-40% of ESBL-producing bacteria that pose resistance to the beta-lactam antibiotics that are normally used to treat them [2].
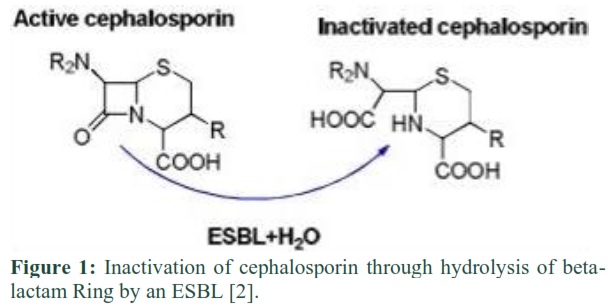
Beta-lactam antibiotics are produced from a wide range of antimicrobial agents, according to literature by Sah [2]. consisting of a 4-atom ring called the beta-lactam ring, within their structure. It is this beta-lactam ring that prevents cell wall synthesis in bacteria, thereby inhibiting their growth. Antibiotics common to this group include penicillin and cephalosporins such as cefotaxime, ceftazidime, monobactams, imipenem and oxymino-monobactam. ESBL+ bacteria hydrolyze the 4-ring beta-lactam ring thereby inactivating it and making it easier for their survival as shown in figure 1.
ESBL+ bacteria tend to fall in one of three classes which are: TEM (Temorina Escherichia coli mutant), SHV (Sulfhydryl variant), and CTX-M (Cefotaximase-Munich) types, with ESBL+ K. pneumoniae strains being predominantly in the SHV-1 group, while most ESBL+ E. coli strains falling in the TEM group [2,11].
ESBL+ K. pneumoniae in particular is a resilient bacterium that has been noted to cause uncomplicated, complicated and recurrent UTIs. In uncomplicated cases of tract infections, symptoms are typically presented in women who are not pregnant, and the symptoms are localized to the lower urinary tract and are either of a dysuria or frequency or urgency nature [4,12].
Complicated cases of UTI caused by ESBL+ K. pneumoniae include complicated pyelonephritis, with 42.8% of cases in North America and Europe being linked to ESBL+ K. pneumoniae [4]. It persists in complicated pyelonephritis because continued antibiotic treatment with antibiotics such as ciprofloxacin in its mild stages, eventually makes the pathogen resistant to carbapenem through its synthesis of carbapenemase This in turn, makes it resistant to almost every beta lactam-based antibiotic available [4,12].
Azadirachta indica (Neem): The benefit of the Neem plant on UTI and other infections
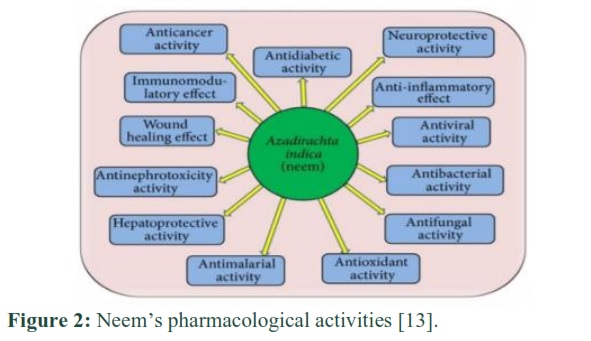
Neem trees have attracted world prominence as holy trees with unique medicinal properties that include immunomodulatory effects, anticancerous effects, hepatoprotective effects amongst others as shown in figure 2.
It is an evergreen tree that grows 15-20 meters in length and belongs to the Meliaceae family that grows in the tropical parts of the globe such as Asia, Africa as well as in the Indian subcontinent and, has an average lifespan of 150-300 years [9,10].
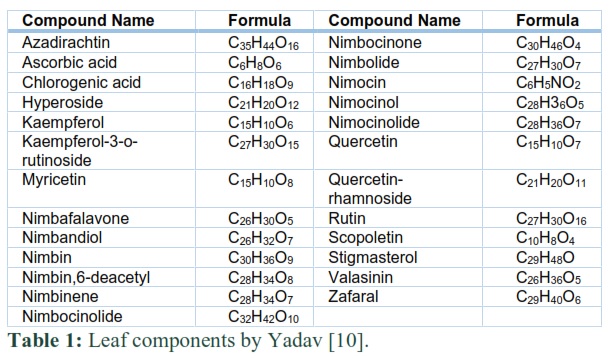
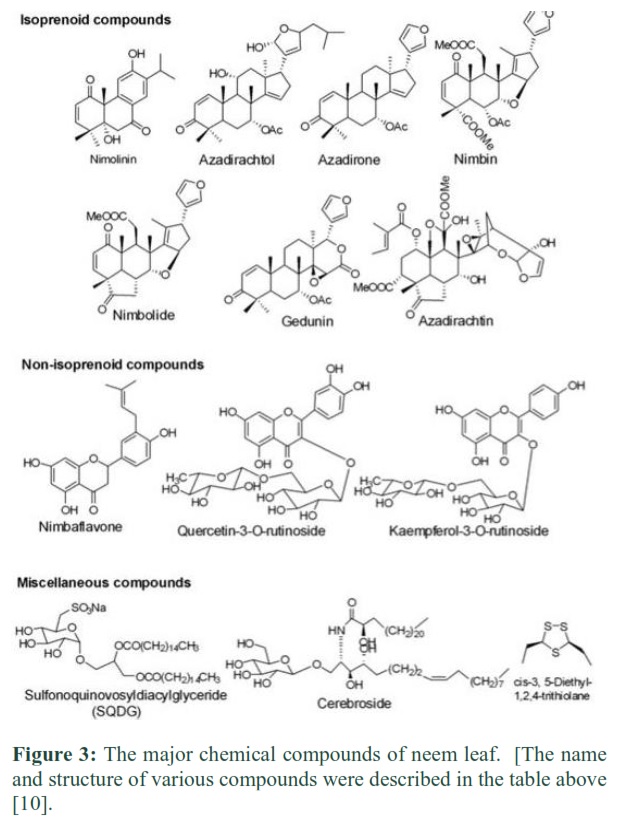
Structurally, neem presents an elaborate array of phytochemicals that are biologically active, chemically diverse and structurally variable, with over 140 compounds that can be isolated from different parts of the tree [9]. Of interest are the neem leaves which have been linked to most of the medicinal properties associated with the tree. Over 60 chemically active compounds that are chemically accounted for have been identified, these are listed in Table1 and Figure 3 [10].
Compounds such as azadirachtin, chlorogenic acid, quercetin, kaempferol/derivatives, myricetin, nimbin, nimbolide, scopoletin and sigmasterol/β-Sitosterol have been shown to possess antioxidant and anti-inflammatory properties, with rutin, being proven to have antihyperglycemic properties as well [10]. Because of this, neem leaves have been used to treat acne, eczema, and other dermatophytic infections successfully [14].
Literature by Yadav [10] has cited links between compounds like azadirachtin to the leaf’s anticancerous properties, with compounds such as Nimbolide being shown to suppress tumor growth by inhibiting cell viability through the induction of programmed cell death (apoptosis). The hepatoprotection of neem leaves was demonstrated through rats, whereby anti-tubercular drug-induced damage was reduced by minimizing alteration of bilirubin, alanine aminotransferase, aspartate aminotransferase, and alkaline phosphatase in vitro serums. In Yadav’s [10], study, antimicrobial, antiviral and antibacterial properties had not yet fully been explored, to explain which compounds were responsible for these effects.
Treatment of ESBL-Positive E. coli and K. pneumoniae using Azadirachta indica (Neem)
The antifungal and antibacterial properties of neem leaves seem to be linked to their antioxidant and anti-inflammatory effects, which in turn, affect bacterial cell processes and inhibit cell growth [10,14].
A study by Mistry [15] revealed that neem extract was active against S. mutans, E. faecalis, and S. aureus. The leaves’ extract was also found to be effective for inhibiting the growth of P. aeruginosa, S. aureus, and Bacillus pumilus, and the effect was compatible with that of antibiotics [16]. A similar study conducted by Parashar, Sutar, and Sanap [17] showed that the optimal effect on E. coli, S. aureus, P. aeruginosa and Bacillus subtilis can be achieved by combining the neem extract with lantana (Lantana Camara) extract made from the plants’ leaves.
Research shows that neem is active against both gram-positive and gram-negative bacteria. A study by Rathod [18] examined the effects of ethanol and aqueous extracts of neem leaves and bark on B. subtilis, S. aureus, K. pneumoniae, and E. coli. It has been found that neem bark was the most effective against the listed bacteria. However, the use of the low concentrations was found to be ineffective as bacteria were resistant to them. Thus, Rathod [18] proved the potential usefulness of neem for primary health care, as it can become an effective alternative to antibiotics. Francine [19] also discussed the importance of extract concentration. The researchers found that the higher the concentration of the extract is, the greater the inhibition zone. In addition, they proved the superiority of fresh leaves and bark over dried parts. Ethanol extracts, in turn, were found to be more effective than aqueous [19].
Along similar lines, Mamman [20] argued that concentration matters when it comes to achieving a significant antibacterial effect. The scholars conducted a study exploring the effects of neem on E. coli, Salmonella spp, and S. aureus. Results have demonstrated that a minimum concentration of 43.75 mg/ml inhibited the growth of E. coli for both the aqueous and methanolic extracts. However, a higher concentration (87.50 mg/ml) was needed to kill the bacteria altogether. To kill E. coli using a methanolic extract, the researchers had to increase the time of exposure and extract concentration (250 mg/ml) [20]. Banna, Parveen, and Iqbal [21], in turn, found that at the concentration of 12.5 mg/mL, ethanolic extract of neem leaves has an inhibitory effect on K. pneumoniae. In this way, both Mamman [20] and Banna [21] vividly demonstrated the importance of measuring the right dosages, concentration, and type of extract to achieve the optimal results.
Recommendations and Future plans:
While neem leaves have shown tremendous therapeutic and medicinal potential, the unfortunate part is research on the effects of neem on antibiotic-resistant bacteria is scarce. Nayim [21] who explored the effects of plants on gram-negative resistant bacteria, including E. coli and K. pneumoniae, conducted one of the studies on the topic.
Interestingly, it has been found that bark extract of neem improved the antibacterial activities of such antibiotics like tetracycline, chloramphenicol, kanamycin, streptomycin, and others. In this way, one may suggest that the combination of commonly used antibiotics with neem extracts can be effective for treating infections caused by multidrug-resistant bacteria. Given the knowledge gap, more research is needed to explore whether neem could be used against ESBL-producing E. coli and K. pneumoniae.
Secondly, based on the case studies explored in this study, age and gender appear to be factors that play a part in the persistence of ESBL+ bacteria in causing UTIs. This needs to be explored more, particularly in relation to how optimal dosages can be achieved in antibiotic treatments for different age and gender demographics, as this will also become a guideline on how to accurately produce neem extracts with the right concentration needed to treat bacterial infections.
Thirdly, research should focus on the mechanisms by which neem antimicrobial/ antibacterial/ antifungal potential works in disrupting bacterial and/or microbial cell growth. Because of knowledge gaps in how these properties are achieved, it then becomes difficult to understand what optimum dosages can be used and what other factors can influence or retard the medicinal properties of neem leaves.
The bean tree has upheld its medicinal prominence for decades, particularly in populations that the tree is indigenous. Indians have used the leaves' extract to heal wounds, eliminate effects of bacterial and fungal infections as well as reduce toxicity in the body. The focus of this particular study was to assess how neem leaf extracts affect ESBL+ bacteria that cause bacteria and while, results gathered from other studies reflected a positive outcome, the knowledge gaps on mechanisms and reactivity to antibiotic-resistant bacteria makes it difficult to fully endorse the use of neem leaf extract as a stand-alone alternative to antibiotic treatment of UTIs. The need for more research that focuses on the influence of factors such as age and gender and how they relate to the resistance of ESBL+ bacteria is apparent. Furthermore, the need for exploring how these factors play a part in determining treatment alternatives is key. However, from this study alone, there is enough evidence to expect an eye-opening outcome from the suggested future investigations. But until then, neem leaf extract must continue to be considered as a viable treatment option for bacterial infections.
I declare that I have no conflict of interest.
References ![]()
- Balighian E, M. Burke. Urinary tract infections in children. Pediatrics in review, (2018); 39(1): 3–12.
- Sah SK, Hemalatha S. Extended spectrum Beta lactamase (ESBL) Mechanism of antibiotic resistance and Epidemiology. International Journal of pharmtechnology and Research, (2015); 7(2): 303-9.
- Hanna-Wakim RH, Ghanem ST, El Helou MW, Khafaja SA, Shaker RA, et al., Epidemiology and characteristics of urinary tract infections in children and adolescents. Frontiers in cellular and infection microbiology, (2015); 5: 45.
- Kang CI, Kim J, Park DW, Kim BN, Ha US et al., Clinical practice guidelines for the antibiotic treatment of community-acquired urinary tract infections. Infection & chemotherapy, (2018); 50(1): 67.
- Al-Momani T, Microbiological study of urinary tract infection in children at Princess Haya Hospital in south of Jordan. Middle East J. Family Medicine, (2006); 3(5): 2.
- Eltai NO, Al Thani AA, Al-Ansari K, Deshmukh AS, Wehedy E, et al., Molecular characterization of extended spectrum β-lactamases enterobacteriaceae causing lower urinary tract infection among pediatric population. Antimicrobial Resistance & Infection Control, (2018); 7(1): 1-9.
- Alshalat ME. Urinary tract infection in home care patients Qatar, Doha. Middle East Journal of Age and Aging, (2014); 11(3): 1-11.
- Al Salman J, Alawi SS, Alyusuf EY. Antibiotic appropriateness for urinary tract infection in the emergency room. Bahrain Medical Bulletin, (2017); 158(5879): 1-5.
- Mahmoud DA, Hassanein NM, Youssef KA, Abou Zeid MA. Antifungal activity of different neem leaf extracts and the nimonol against some important human pathogens. Brazilian Journal of Microbiology, (2011). 42(3): 1007-1016.
- Yadav DK, Bharitkar YP, Chatterjee K, Ghosh M, Mondal NB, Swarnakar S. Importance of Neem Leaf: An insight into its role in combating diseases. Indian Journal of Experimental Biology, (2016); 54(11): 708-18.
- Rupp ME, Fey PD. Extended spectrum β-lactamase (ESBL)-producing Enterobacteriaceae. Drugs, (2003); 63(4): 353-365.
- Paczosa MK, Mecsas J. Klebsiella pneumoniae: going on the offense with a strong defense. Microbiology and Molecular Biology Reviews, (2016); 80(3): 629-661.
- Shareef M, Akhtar MS. Neem (Azadirachta indica) and its potential for safeguarding health, prevention and treatment of diseases. Matrix Science Medica, (2018); 2(1): 04-08.
- Faujdar SS, Bisht D, Sharma A. Antibacterial potential of neem (Azadirachta indica) against uropathogens producing beta-lactamase enzymes: A clue to future antibacterial agent? Biomedical and Biotechnology Research Journal (BBRJ), (2020). 4(3): 232.
- Mistry KS, Sanghvi Z, Parmar G, Shah S. The antimicrobial activity of Azadirachta indica, Mimusops elengi, Tinospora cardifolia, Ocimum sanctum and 2% chlorhexidine gluconate on common endodontic pathogens: An in vitro study. European journal of dentistry, (2014); 8(2): 172-177.
- Brindha S, Maragathavalli S, Kaviyarasi NS, Annadurai BB, Gangwar SK. Antimicrobial activity in leaf extract of neem (Azadirachta indica linn). International Journal of Science and Nature, (2012); 3(1): 110-113.
- Parashar G, Sutar N, Sanap S. Antibacterial activity of mixture of leaf extracts of neem (Azadirachta indica linn.) and Tantani (Lantana camara). International Journal of Pharmaceutical Sciences and Research, (2018); 9(6): 2545-2549.
- Rathod GP. In vitro Antibacterial study of two commonly used medicinal plants in Ayurveda: Neem (Azadirachta indica L.) and Tulsi (Ocimum sanctum L.). drugs, (2010); 9: 10.
- Francine U, Jeannette U, Pierre RJ. Assessment of antibacterial activity of neem plant (Azadirachta indica) on Staphylococcus aureus and Escherichia coli. Journal of Medicinal Plants Studies, (2015); 3(4): 85-91.
- Mamman PH. Antibacterial effects of crude extract of Azadirachta indica against Escherichia coli, Salmonella spp and Staphylococcus aureus. International Journal of Medicine and Medical Sciences, (2013); 5(1): 14-18.
- Banna QR, Parveen F, Iqbal MJ. Growth inhibitory effect of ethanolic neem leaves extract on Klebsiella, Salmonella and Staphylococcus aureus. Bangladesh Journal of Pharmacology, (2014); 9(3): 347-350.
- Nayim P. Antibacterial and antibiotic-potentiating activities of thirteen cameroonian edible plants against gram-negative resistant phenotypes. The Scientific World Journal, (2018); 4020294.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0