

Full Length Research Article
Validity of anti-nuclear antibodies, double strand DNA antibodies and other parameters in autoimmune hypoparathyroidism
Hind H. Al-Ammiri1*, Tharwa H. Hasan Al-Tai2, Ali A. A. Mahdi3
Adv. life sci., vol. 11, no. 1, pp. 72-76, February 2024
*– Corresponding Author: Hind H. Al-Ammiri (Dr.hindhamid@covm.Uobaghdad.edu.iq)
Authors' Affiliations
2. Clinical Communicable Diseases Research Unit, College of Medicine, University of Baghdad – Iraq
3. Medical Lab. Science Technology, College of Health and medical Technology, Middle Technical University – Iraq
[Date Received: 27/07/2022; Date Revised: 06/09/2023; Date Published: 25/02/2024]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Hypoparathyroidism is the destruction of the parathyroid gland by the immune system, as part of a multiple endocrine insufficiency syndrome. Tissue resistance to PTH's activities can occur in rare cases, resulting in hypoparathyroidism with increased PTH levels. Hypothyroidism is more common in females than males. 1,25-dihydroxyvitamin D3 (active vitamin D) levels must be evaluated to rule out vitamin D deficiency as a contributor to or cause of hypocalcemia. Hypocalcemia and phosphatemia are common symptoms of hypoparathyroidism. Antinuclear antibodies (ANA) and double strand DNA (DsDNA) are the important biomarkers for diagnosis and prognosis of patients with autoimmune diseases. ANA and DsDNA occur in different endocrine disorders including thyroid disorders like hypoparathyroidism.
Methods: Thirty Hypoparathyroidism patients with age range 21-74 years with (20 female and 10 male) were attending international Baghdad Medical Hospital, during the period from December 2019 to February 2021 and thirty apparently healthy were chosen as healthy control groups respectively. For these two study groups, the blood samples were collected to evaluate the serum level of serum phosphorus, calcitonin, Calcium, Vitamin D3, DsDNA and ANA. The type of kits used for serum DsDNA and ANA in humans were an indirect enzyme immunoassay (ELISA) and the kits for serum level of serum Vitamin D3 and calcitonins were a sandwich ELISA. Finally, these kits for the calcium and phosphorus inorganic Colorimetric method were used.
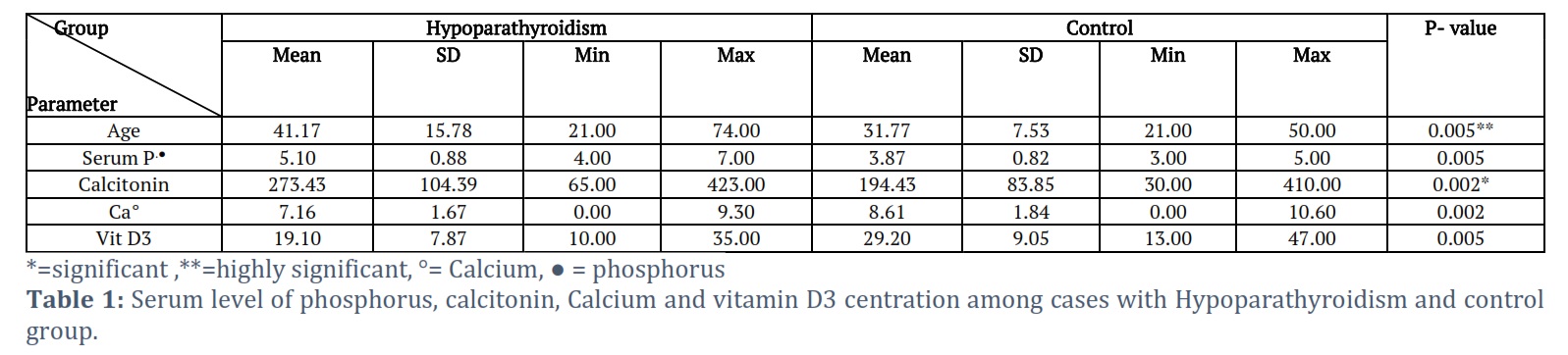
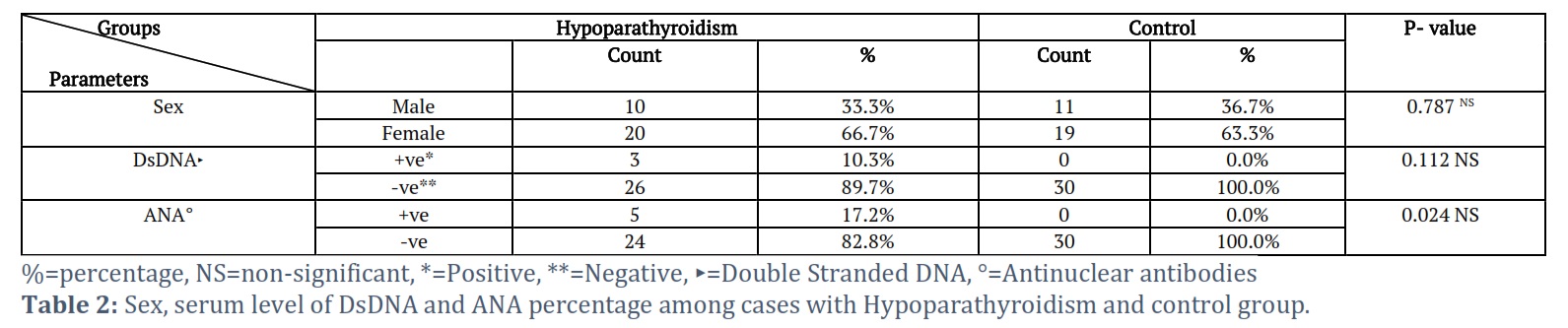
Results: Using Student's t-test, the present study's data revealed a statistically significant difference in the mean of age group cases and controls (P=0.005), as well as a statistically significant difference in serum mean values of each Serum phosphorus (P=0.005), calcitonin (P=0.005), calcium (P=0.002), and vitamin D3 centration (P=0.005) between these two groups . By using Chi-square test sex was not significant between hypoparathyroid and control (P=0.787) and DsDNA was not significantly more positive in hypoparathyroid subjects than control (P=0.112); while ANA was significant (P=0.024).
Conclusion: The study sheds light on the necessity to screen the hypo parathyroid patients for vitamin D, calcium and phosphorous levels and calcitonin for better prognosis of patients and for each of antinuclear antibodies (ANA) and double strand DNA (DsDNA).
Keywords: Hypoparathyroidism; Phosphate; Calcium; Calcitonin; Vitamin D; ANA; DsDNA
Introduction![]()
Primary hypothyroidism is the second most common endocrine disease worldwide after diabetes mellitus and is characterized by thyroid hormone deficiency. Accidental damage to or removal of the parathyroid glands during neck surgery are the most common causes of hypoparathyroidism. Years after a neck operation, it is possible [1, 2]. To follow this issue, most head and neck surgeons measure calcium and PTH levels both during and after surgery [3].
Most patients with hypoparathyroidism present with hypocalcemia, the etiology of hypocalcemia is obvious in certain individuals, such as those with acute pancreatitis, sepsis, or other urgent illnesses, and therapy without further investigation is necessary [4]. The intensity, extent, and pace of the development of hypocalcemia symptoms vary; therefore, it’s critical for these people to get their vitamin D and magnesium levels back to normal. PTH, phosphorus, 25-hydroxyvitamin D, and 1, 25-dihydroxyvitamin D levels in the blood can help distinguish between illnesses that cause hypocalcemia. Long-term management of hypoparathyroidism should include Vitamin D analogs are essential, and dietary modifications are typically used as well [4].
In contrast to the high levels in hypoparathyroidism, intact PTH levels are raised in typical vitamin D insufficiency, while phosphorous levels in the blood are low or at the low end of the normal range [5]. Hypocalcemia, or low albumin-corrected total calcium or ionized calcium levels in the blood, is a common clinical phenomenon that can be caused by a variety of factors. Low parathyroid hormone (PTH) synthesis or receptor activation, insufficient vitamin D availability, or vitamin D receptor activity are all causes of hypocalcemia [1]. Thyroid disorders were considered as the common causes of autoimmune thyroid; in which self-antigen recognized as a foreign antigen result in autoantibodies destructed thyroid cells [6]. Antinuclear antibodies (ANA) and double-stranded DNA (DsDNA) are two of the most performed screening tests for the detection of autoimmune diseases. They are found in a wide array of autoimmune diseases affecting many endocrine organs, such as autoimmune thyroid disease (AITD) like hyperparathyroidism [7].
Methods![]()
Patients study groups
Ethical agreement: The Baghdad medical microbiological Laboratories/ University of Baghdad and the college of medical technology/ middle technical university both gave their approval for this study.
Thirty Hypoparathyroidism patients with age range 21-74 years with (20 female and 10 male) were attending international Baghdad Medical Hospital, during the period from December 2019 to February 2021.
Thirty apparently healthy were chosen as healthy control groups respectively. Blood samples were taken from these two study groups in order to measure the levels of serum phosphorus, calcitonin, calcium, vitamin D3, dsDNA, and ANA using indirect and sandwich ELISA techniques as well as colorimeter methods.
Kits and reagents
The ANA Screen ELISA test system is an ELISA that detects IgG class antibodies to ANA in human serum (a titer above 1:160 as positive) (AbNOVA, Germany). The Anti-dsDNA Screen (A,G,M) indirect ELISA was used to determine the quantity and quality of IgG, IgA, and IgM antibodies against double-stranded DNA (dsDNA) in human serum; With standard results dsDNA (<30.0 IU/mL (negative) >75.0 IU/mL (positive)).
Also, for the Calcium Total Colorimetric method and Phosphorus Inorganic Colorimetric method (LINEAR CHEMICALS; SPAIN) the standard results (8.5-10.5mg/dl and 3-4.5mg/dl) respectively.
The Human Vitamin D3 (VD3) ELISA Kit, this kit employs Double Antibody Sandwich Technique; the standard result is 30-100 ng/ml (MYBIOSOURCE; USA). And even the Human Calcitonin (CT) ELISA Kit, for determining the amounts of human calcitonin (CT) in serum, the standard result is 130-190 ng/l. Finally, the quantitative sandwich enzyme immunoassay approach is used in this experiment. (CUSABIO).
Statistical analysis:-The statistical analysis was carried out using the SPSS statistics software for Social Sciences (version 20.0 for Windows, SPSS, Chicago, IL, USA).To represent quantitative data, the mean and standard deviation are utilized. To convey qualitative data, utilize count and percentage. To determine whether two groups vary in any way, the students' t-test was used. The Chi-square test was used to assess the association between qualitative data. Finally, it was decided that a (P value) lower than 0.05 was statistically significant.
Results![]()
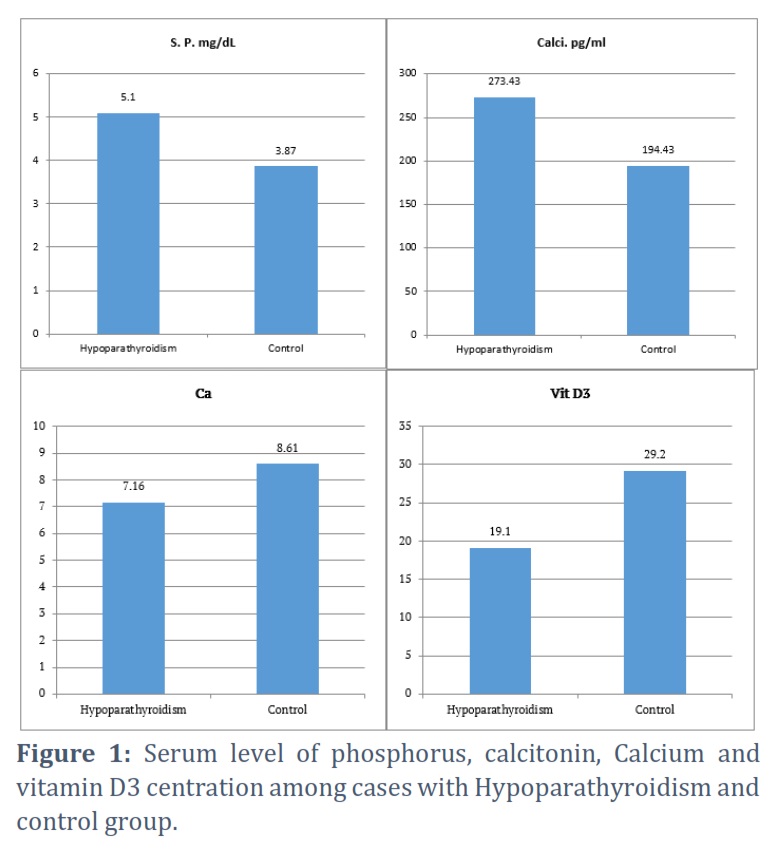
Thirty hypoparathyroidism subjects were selected and compared with 30 apparently healthy subjects. The results of this study revealed a statistically significant difference in the mean of age group cases and controls (P=0.005), as well as statistically significant differences in serum mean values of each Serum phosphorus (P=0.005), calcitonin (P=0.005), calcium (P=0.002), and vitamin D3 centration (P=0.005) between these two groups (Table 1), (Figure 1). By using the Chi-square test Gender was not significant between hypoparathyroid and control (P=0.787) and DsDNA was not significantly more positive in hypoparathyroid subjects than control (P=0.112); while ANA was significant (P=0.024).
Figures & Tables
This finding was in line with the findings of numerous studies, including those by Haden et al., [8], who report that there were no sex differences in the set-point, slope at the set-point, or maximal or minimal PTH levels in men and women during induced hypo and/or parathyroidism (P = 0.787) during dynamic testing. But hypothyroidism is more common in females than males [18]. Age was substantially different from control in this study (P = 0.005); however, using the Chi-square test, sex was determined to be statistically significant because of that. An integrated measure of PTH changes as a function of time was identified in older patients. The maximum PTH values for the four parameter sigmoidal curves were around 25% higher in older women than in younger women, but this was not statistically significant due to the small amount of data and large interindividual variability in PTH responses. However, despite the roughly twofold differences in this parameter, the same causes are most likely to blame for the lack of a significant increase in the minimal PTH level of these curves for older vs. younger women.
Ledger et al., [9] found similar results using a slightly modified procedure to induce hypocalcemia [8]. In both men and women, serum parathyroid hormone (PTH) levels rise with age, and this has been linked to a decline in renal function as people age [10].
Hypocalcemia, or low albumin-corrected total calcium or ionized calcium levels in the blood, is a common clinical phenomenon that can be caused by a variety of factors. Insufficient parathyroid hormone (PTH) secretion or receptor activation, insufficient vitamin D supply or receptor activity, aberrant magnesium metabolism, or clinical circumstances in which many variables (e.g., pancreatitis, sepsis, and severe illness) play a role in producing hypocalcemia. [1]. In the current study, calcium and vitamin D3 significantly varied from the control group (P = 0.002 and P = 0.005, respectively). Numerous investigations have shown that hypoparathyroidism causes hypocalcemia because there is inadequate PTH production to sustain renal 1-hydroxylase activity, mobilize calcium from bone, and reabsorb calcium from the distal nephron. The body does not make enough 1,25-dihydroxyvitamin D (1,25[OH]2 vitamin D), which is necessary for appropriate calcium absorption in the intestine [1,11,12].
Aging is related to an increase in the integrated PTH secretory response to variations in blood calcium in both women and men, regardless of changes in vitamin D or renal function. The Cai/iPTH/iPTHpoint remained the same. The biological relevance of these modest increases in integrated iPTH levels during dynamic testing in older, healthy men and women is unknown [8]. Hypoparathyroidism can also lead to hyperphosphatemia. There were significant differences in serum phosphorus between patients and controls in this study (P = 0.005), which was in line with the results of Shoback et al., who found that hyperphosphatemia is asymptomatic and causes ectopic mineralization and clinical repercussions in soft tissues of the vascular, neurological, renal, and other organs over time, which can permanently damage their function. [13]. In hypoparathyroidism, hypercalcemic episodes in the context of hyperphosphatemia increase the risk of ectopic mineralization in the kidney and hasten the onset of chronic kidney disease (CKD) [14]. The involvement of calciophosphotropic hormones like PTH in tight-junction permeability control has gotten a lot of press recently. According to functional data, PTH signaling and altered paracellular transports in the PT are connected. The PT reabsorption of paracellular solutes was inhibited in rats after an acute infusion of PTH [15].
In this investigation, there were statistically significant variations in calcitonin levels between patients and controls (P = 0.005). Although active vitamin D is typically thought of as a calciotropic hormone, Lee et al., found that it is both a phospho and calciotropic hormone that promotes intestine absorption to raise serum calcium and phosphate levels. It can better grasp how calcium and phosphate are regulated in the kidney in health and disease by comprehending the molecular mechanisms that allow calcium and phosphate to cross the PT in the presence and absence of these hormones [15].
On the other hand, in this study the DsDNA was not significantly, but more positive in hypoparathyroid subjects than control (P=0.112); while ANA was significant (P=0.024). The study's main finding was that patients had greater frequencies of ANA and antibodies to dsDNA than controls, but antibodies against dsDNA had only been occasionally observed. This result seems to be in agreement with numerous studies that describe this. As a result, studies show those patients who produce high-affinity antibodies to dsDNA and ANA are more likely to develop autoimmune illness [16].
The prevalence of ANA in newly developed subclinical hypoparathyroid patients was observed to be 45% as compared to 10% in normal population; this clearly shows that subclinical hypoparathyroid patients are more prone to develop autoimmune disease. Moreover, the numbers of positive cases in male and female population are more or less similar in both categories. There is a significant increase in the number of females showing positivity for ANA in subclinical hypoparathyroidism (66%).
In case of patients with hypoparathyroid autoimmune diseases; they must undergo detection of vitamin D, calcium and phosphorous levels and calcitonin for early diagnosis and Anti-nuclear antibodies (ANA) and double strand DNA (DsDNA) are the important biomarkers for diagnosis and prognosis of patients with autoimmune diseases.
Conflict of Interest
The authors declare that there is no conflict of interest.
Hind H. Al-Ammiri / study conception, analysis design, interpretation of results and article writing.
Tharwa H. Hasan AL-tai / study conception, statistical data analysis & critical revision.
Ali A.A. Mahdi / acquisition of data collection and critical revision.
![]() References
References
- Shobac D. Clinical practice. Hypoparathyroidism. New England Journal of Medicine, (2008); 359(4): 391-403.
- Radhi SM, Essam FA, and Muqdad AA. Evolution of Thyroid Autoantibodies and Thyroid Parameters in Iraqi Hypothyroidism Patients. Iraqi journal of biotechnology, (2022); 21(2):172-177.
- Udelsman R, Pasieka JL, Sturgeon C, Young J and Clark OH. Surgery for asymptomatic primary hyperparathyroidism: proceedings of the third international workshop. Journal Clinical Endocrinology and Metabolism, (2009); 94(2): 366-72.
- Michels TC and Kelly KM. Parathyroid disorders. American family physician Journal, (2013); 88(4): 249-57.
- Thakker R. Genetics of endocrine and metabolic disorders: parathyroid. Reviews Endocrine and Metabolic Disorders, (2004); 5(1): 37-51.
- Al-Mofarji ST, Jasim HM, and Mohammed SB. Thyroid Hormones and Autoantibodies in Iraqi Hyperthyroid Patients. Al-Nahrain Journal of Science, (2023); 26 (2), 56-59.
- Agmon-Levin N, Damoiseaux J, Kallenberg C, Sack U, Witte T, Herold,M ,and Shoenfeld Y.International recommendations for the assessment of autoantibodies to cellular antigens referred to as anti-nuclear antibodies. Annals of the rheumatic diseases,(2014); 73(1), 17-23.
- Haden ST, Brown EM, Hurwitz S, Scott J and Fuleihan GEH. The effects of age and gender on parathyroid hormone dynamics. Clinical endocrinology, (2000); 52(3): 329-338.
- Ledger GA, Burritt MF, Kao PC, O'Fallon WM, Riggs BL, and Khosla S. Abnormalities of parathyroid hormone secretion in elderly women that are reversible by short term therapy with 1, 25-dihydroxyvitamin D3. The Journal of Clinical Endocrinology & Metabolism, (1994); 79(1): 211-216.
- Need AG, O’loughlin PD, Morris HA, Horowitz M and Nordin BC. The effects of age and other variables on serum parathyroid hormone in postmenopausal women attending an osteoporosis center. The Journal of Clinical Endocrinology & Metabolism, (2004); 89(4): 1646-1649.
- Leong A, Rehman W, Dastani Z, Greenwood C, Timpson N, Langsetmo L, Berger C, Metastroke, FU L and Wong BY. The causal effect of vitamin D binding protein (DBP) levels on calcemic and cardiometabolic diseases: a Mendelian randomization study. PLoS Medicine, (2014); 11: e1001751.
- Marx S. Hyperparathyroid and hypoparathyroid disorders. New England Journal of Medicine, (2001); 344(9): 696-696.
- Shoback DM, Bilezikian JP, Costa AG, Dempster D, Dralle H, Khan AA, Peacoc M, Raffaelli M, Silva BC and Thakker RV. Presentation of hypoparathyroidism: etiologies and clinical features. The Journal of Clinical Endocrinology and Metabolism, (2016); 101(6): 2300-2312.
- Boyce AM, Shawker TH, Hill SC, Choyke PL, Hill MC, James R, Yovetich NA, Collins MT and Gafni RI. Ultrasound is superior to computed tomography for assessment of medullary nephrocalcinosis in hypoparathyroidism. The Journal of Clinical Endocrinology and Metabolism, (2013); 98(3): 989-994.
- Lee JJ, Plain A, Beggs MR, Dimke H and Alexander RT. Effects of phospho-and calciotropic hormones on electrolyte transport in the proximal tubule. F1000 Research, (2017); 3;6:1797.
- Kälkner KM, Rönnblom L, Karlsson Parra AK, Bengtsson M, Olsson Y, and Oberg K. Antibodies against double-stranded DNA and development of polymyositis during treatment with interferon. QJM: monthly journal of the Association of Physicians, (1998); 91(6): 393-399.
- Uchida S, Maruyama T, Kagami M, Miki F, Hihara H, Katakura S, and Tanaka M. Impact of borderline–subclinical hypothyroidism on subsequent pregnancy outcome in women with unexplained recurrent pregnancy loss. Journal of Obstetrics and Gynaecology Research, (2017); 43(6): 1014-1020.
- Al-Jowari SA. Comparative Investigation of Thyroid Autoantibodies Between Type 1 and Type 2 Diabetes Mellitus Patients in Baghdad City. Iraqi Journal of Science, (2022); 58 (2B): 815–819.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0